
OCD vs Anxiety: What Is the Difference and Why It Matters
Written by Armaan Raheja, Founder of breakOCD | Clinically reviewed by Dr. Sachi Pandya, Psychologist, Mumbai
You were told it was anxiety. The treatment did not help the way it should have. And now you are wondering if something else is happening.
OCD and anxiety are often confused. The distinction is not about severity. It determines whether your treatment will actually work.
If you have been told you have anxiety and the treatment has not helped the way it should, there is a possibility that something more specific is happening. Not because the diagnosis was dishonest, but because OCD and anxiety share enough surface features that they are frequently mistaken for each other, even by experienced clinicians.
The distinction between OCD and anxiety is not a matter of severity or sensitivity. It is a clinical distinction that determines whether the treatment you receive will actually work. Anxiety and OCD respond to different therapeutic approaches. Getting the wrong one does not just fail to help. It can make things significantly worse.
This article explains what separates OCD from anxiety, why the confusion is so common in India, and what the right path forward looks like for each condition.
What Is Anxiety?
Anxiety is the body and mind's response to perceived threat or uncertainty. It is a normal human experience that becomes a clinical concern when it is disproportionate to the situation, persistent, and significantly impairing daily life.
Clinical anxiety disorders include generalised anxiety disorder, social anxiety disorder, panic disorder, specific phobias, and health anxiety, among others. What these conditions share is a core mechanism: the brain treats certain situations or stimuli as dangerous and generates a fear response that is out of proportion to the actual risk.
Anxiety tends to be future-focused. The person worries about what might go wrong, how they might fail to cope, or what bad things might happen. When the feared situation resolves or passes, the anxiety typically eases. Reassurance from a trusted person helps and tends to produce lasting relief. Avoidance reduces the anxiety in the moment.
Generalised anxiety disorder, the most common anxiety diagnosis, involves persistent, excessive worry across multiple domains of life. The worry feels difficult to control but it is fundamentally about real-world concerns: work, health, relationships, finances, safety. The content of the worry connects to genuine uncertainties in the person's life.
What Is OCD?
Obsessive-Compulsive Disorder is defined in the DSM-5-TR by the presence of obsessions, compulsions, or both, that are time-consuming, cause significant distress, and impair daily functioning. As of 2013, OCD was reclassified out of the anxiety disorders category into its own separate category in the DSM, reflecting growing clinical evidence that it is a distinct condition with a different underlying mechanism and a different optimal treatment pathway.
Obsessions are intrusive, unwanted thoughts, images, urges, or doubts that arrive repeatedly and cause significant distress. They are experienced as ego-dystonic: they feel foreign to the person's sense of self, often horrifying or shameful, and completely unwanted. Obsessions can range across various themes, usually around health, safety, identity, religion, or the fear of doing harm. Harm obsessions, religious obsessions, sexual intrusive thoughts, and relationship doubt are among the most common and least recognised forms of OCD in India.
Compulsions are the behavioural or mental acts performed in response to the obsession to reduce anxiety or prevent a feared outcome. They provide temporary relief. Within minutes to hours, the obsessive doubt returns and the compulsion is needed again.
Why OCD was reclassified
In 2013, OCD was moved out of the anxiety disorders category in the DSM-5 and into its own separate category. This reflects clinical evidence that OCD has a distinct mechanism and a distinct optimal treatment pathway.
This reclassification matters for patients because it means OCD is not a more severe form of anxiety. It is a different condition that requires a different treatment. Standard anxiety treatment applied to OCD often fails, and sometimes makes things worse.
The Key Differences Between OCD and Anxiety
The obsession-compulsion cycle
This is the fundamental clinical distinction between OCD and anxiety. In OCD, a specific intrusive thought triggers anxiety, which drives a specific compulsion to neutralise the threat. The compulsion provides temporary relief. The doubt returns stronger. The compulsion is performed again. This is the defining loop of OCD and it is absent in generalised anxiety disorder.
In anxiety, worry is diffuse and future-focused. It does not follow the precise trigger-obsession-compulsion-relief-return pattern. A person with generalised anxiety worries broadly about real-world concerns. They may develop avoidance behaviours, but they do not perform specific rituals in response to specific intrusive thoughts. When a person is stuck in a cycle of a specific thought driving a specific behaviour driving brief relief driving the return of the thought, that is OCD, not anxiety.
Understanding this cycle is critical for treatment because ERP therapy specifically targets the compulsion response. It works by breaking the link between the obsessive trigger and the compulsive response, teaching the brain that the feared outcome does not require a compulsion to manage. No amount of anxiety treatment addresses this mechanism because anxiety treatment is not designed to interrupt this specific cycle.
The OCD cycle in plain language
Intrusive thought arrives
Anxiety spikes
Compulsion performed to neutralise the threat (physical or mental)
Brief relief
Doubt returns stronger. The cycle repeats.
This cycle is absent in generalised anxiety disorder. It is the reason OCD requires a specific treatment and why anxiety treatment does not work for it.
The content of the fear
Anxiety fears tend to be broad and about realistic possibilities in proportion to actual life circumstances. A person with generalised anxiety worries about their health, their job, their relationships, or their finances. These are genuine concerns that many people share.
OCD obsessions are ego-dystonic: they are thoughts the person does not want, that contradict their values, and that feel completely alien to who they are. A person who deeply values their faith has blasphemous intrusive thoughts during prayer. A person who would never harm anyone has thoughts about hurting the people they love most. A person who is deeply committed to their relationship has relentless doubt about whether they love their partner. And many more. OCD has many themes. The content of OCD obsessions tends to attack exactly what matters most to the person. This is not a coincidence. It is the mechanism.
Whether reassurance works
In generalised anxiety, reassurance from a trusted person tends to produce lasting relief. You tell someone with health anxiety that their test results are normal and they feel better. The relief is meaningful and sustained.
In OCD, reassurance provides temporary relief that disappears within minutes to hours. The person asks the same question again, slightly differently. No answer is ever final enough. This is because OCD is not really asking a question. It is seeking certainty, and certainty is exactly what OCD demands and never allows to arrive. Reassurance feeds the cycle rather than breaking it.
This distinction is clinically critical because it determines whether reassurance from family members, friends, or clinicians is helpful or harmful. In OCD, it is harmful. In anxiety, it can be genuinely therapeutic.
Reassurance in OCD is a compulsion
In anxiety, reassurance produces lasting relief. In OCD, reassurance is a compulsion. It works briefly and then the doubt returns stronger, now having learned that asking was a necessary response to the threat.
This is why reassurance from family members, however loving, maintains the OCD cycle rather than breaking it. And why gradually reducing reassurance-giving is part of effective OCD treatment.
What makes things worse
For anxiety, many standard therapeutic approaches help. Talking about worries, seeking reassurance, avoiding triggers, and practising relaxation techniques can all reduce anxiety symptoms meaningfully in the short term.
For OCD, these same strategies tend to make things worse. Talking through an obsessive doubt repeatedly is a form of reassurance-seeking that strengthens the cycle. Avoiding triggers confirms to the brain that the threat is real and dangerous. Trying to relax through a compulsion provides relief that maintains the pattern. This is why so many people with OCD who receive standard anxiety treatment do not improve and often feel more confused and hopeless.
The treatment
Anxiety disorders respond well to a range of evidence-based treatments including cognitive behavioural therapy, medication, mindfulness-based approaches, and in some cases exposure therapy for specific phobias.
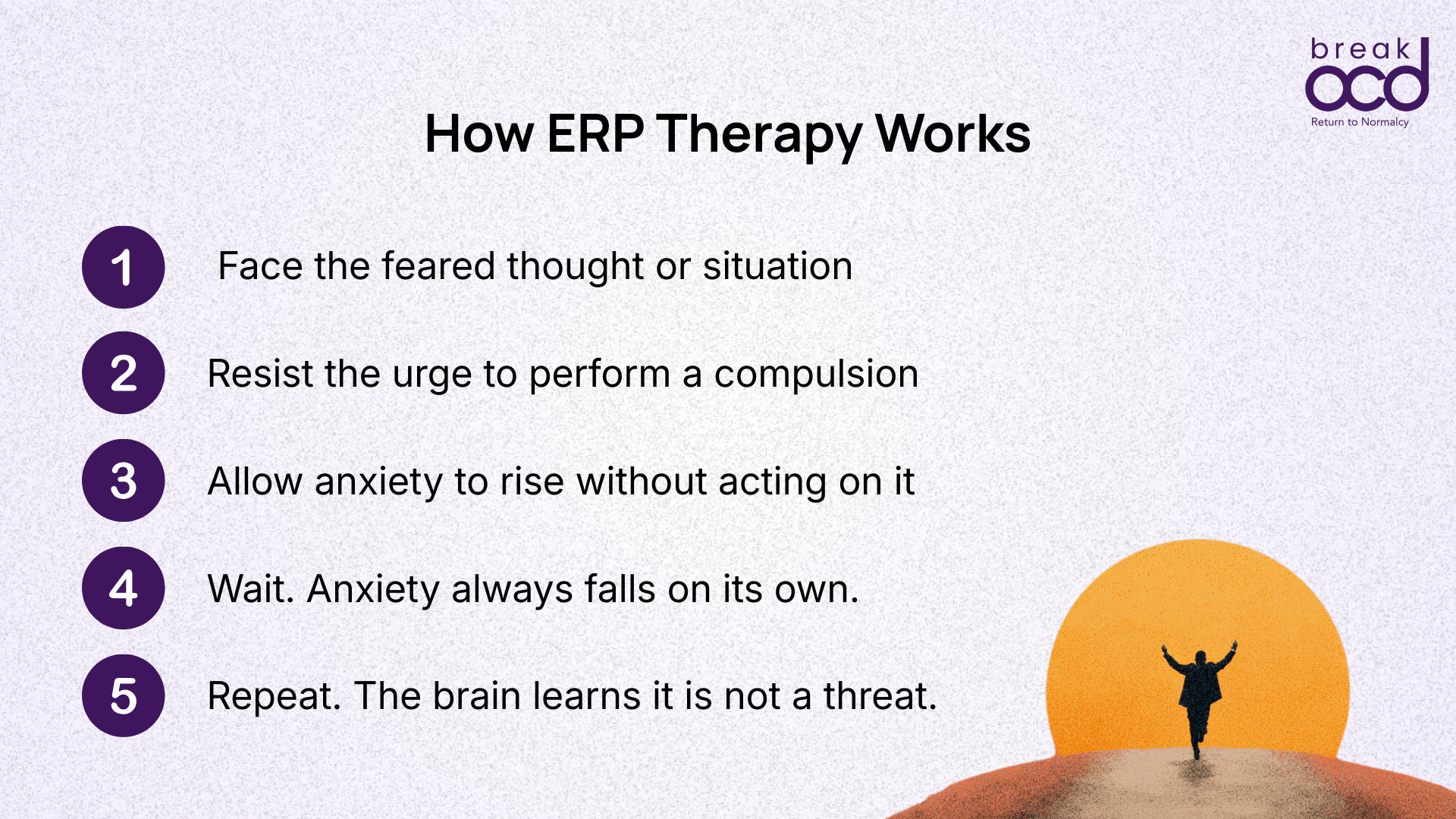
OCD requires a specific form of treatment: Exposure and Response Prevention therapy, known as ERP. ERP works by deliberately exposing the person to their obsessive trigger and then preventing the compulsive response, teaching the brain that the feared outcome does not require a compulsion to manage. ERP does not work by reducing anxiety through reassurance or avoidance. It works by building tolerance for uncertainty. This approach is counterintuitive and it is the specific reason why general anxiety treatment does not work for OCD. ERP is not simply exposure therapy. It is a clinically precise approach designed around how OCD specifically maintains itself.
Why the right treatment matters
ERP therapy for OCD does not work by reducing anxiety through reassurance or avoidance. It works by building tolerance for uncertainty. This is why general anxiety therapy does not work for OCD and why getting the right diagnosis changes everything.
Most people with OCD who receive general anxiety treatment do not improve. This is not a reflection of how hard they are trying. It is a reflection of receiving treatment designed for a different condition.
Why OCD Is So Frequently Misdiagnosed as Anxiety in India
The misdiagnosis of OCD as anxiety in India is not a failure of individual clinicians. It is a systemic problem rooted in the limited availability of OCD-specific training, the cultural context in which OCD presents, and the significant overlap in how the two conditions appear on the surface.
Research published in the Indian Journal of Psychiatry by Janardhan Reddy and colleagues identifies OCD as one of the most chronically underdiagnosed conditions in India. The average gap between onset of symptoms and correct diagnosis is estimated at 11 to 17 years. Much of this time is spent in treatment for anxiety or depression that does not address the underlying OCD.
The surface overlap
Both OCD and anxiety involve significant distress. Both involve avoidance. Both involve repetitive negative thinking. Both can cause physical symptoms including racing heart, disturbed sleep, and difficulty concentrating. In a clinical assessment that focuses on symptoms rather than mechanism, the two can look identical.
The person with OCD who presents to a general practitioner is not describing their intrusive thoughts in detail. They are describing the anxiety those thoughts produce. They say they are anxious all the time, that they cannot stop worrying, that they have been avoiding certain situations. A clinician without specific OCD training hears this and correctly identifies anxiety. The OCD underneath remains invisible.
The shame of disclosure
In India, the shame attached to OCD symptoms creates a specific barrier to accurate diagnosis that does not exist to the same degree in other cultural contexts. A person with harm OCD is not going to walk into a doctor's office and describe their intrusive thoughts about hurting a family member. A person with religious OCD is not going to describe blasphemous thoughts to a clinician they have just met. A person with sexual intrusive thoughts is not going to disclose the content of those thoughts in an initial consultation.
Instead they describe the surface symptoms. The anxiety. The difficulty functioning. The rituals they have developed to manage a fear they cannot name. Without the specific content of the obsessions, the OCD goes unrecognised and the anxiety label gets applied.
The wrong treatment reinforces the wrong belief
When a person with OCD receives treatment for generalised anxiety that does not help, two things often happen. First, the treatment approach, which may include reassurance, cognitive restructuring, and relaxation techniques, actively maintains or worsens the OCD cycle because these are the strategies OCD exploits rather than resists. Second, the person concludes that their condition is untreatable, that they are unusually resistant to treatment, or that something is fundamentally wrong with them beyond what any diagnosis can explain.
This experience, of seeking help, receiving the wrong treatment, not improving, and losing hope, is one of the most common journeys for people with OCD in India. It is also entirely preventable with accurate diagnosis and OCD-specific treatment.
Can You Have Both OCD and Anxiety?
Yes. Comorbidity between OCD and anxiety disorders is common. Research consistently shows that a significant proportion of people with OCD also meet criteria for at least one anxiety disorder, most commonly generalised anxiety disorder or social anxiety disorder.
When both conditions are present, the treatment picture is more complex but not more hopeless. ERP remains the primary treatment for the OCD component. The anxiety component may be addressed concurrently or sequentially depending on which is more impairing.
The important clinical point is that treating the anxiety without addressing the OCD will produce partial and unstable improvement. The OCD component needs to be identified and treated specifically. A clinician who understands both conditions can develop a treatment plan that addresses each appropriately.
Signs That What You Have Might Be OCD Rather Than Anxiety
It may be worth seeking an OCD-specific assessment if several of the following apply to you.
You have specific recurring thoughts, images, or doubts that feel intrusive, unwanted, and completely alien to who you are.
You perform specific behaviours/rituals or mental acts in response to these thoughts to reduce anxiety or prevent something bad from happening.
The relief from these behaviours lasts only minutes before the doubt returns, often stronger than before.
Reassurance from others helps only briefly and the same question keeps returning in new forms.
You have received anxiety treatment that has not helped in the way you expected.
You carry intense shame about the content of your thoughts and have never disclosed them fully to a clinician.
Your daily functioning is significantly affected by the time spent on rituals or mental checking.
Consider an OCD-specific assessment if any of these apply
You have specific intrusive thoughts that feel alien to who you are and that you never asked for
You perform specific rituals or mental acts in response to these thoughts
Reassurance provides only brief relief before the doubt returns
You have received anxiety treatment that has not helped in the way you expected
You carry shame about the content of your thoughts and have not disclosed them fully to a clinician
Seeking the Right Help
If you suspect OCD may be a better explanation for your experience than anxiety, the most important next step is seeking an assessment from a clinician who has specific training in OCD. Not all mental health professionals are trained in OCD, and a clinician who does not understand the distinction between OCD and anxiety may inadvertently provide treatment that makes things worse.
When seeking an assessment, be as specific as possible about your experience. Describe the content of your intrusive thoughts, even if it feels shameful. Describe the specific behaviours or mental acts you perform in response. Describe how long the relief lasts before the doubt returns. An OCD-trained clinician will not judge the content of your thoughts. The content is diagnostically important and will help them understand your specific pattern.
Ask explicitly whether the clinician has experience treating OCD with ERP. This distinction matters significantly for outcomes. ERP delivered by a clinician trained in OCD produces meaningfully better results than general anxiety treatment applied to OCD.
Frequently Asked Questions
I have been diagnosed with anxiety for years. Could it actually be OCD?
Possibly, and it is worth exploring. The most useful questions to ask yourself are: do you have specific intrusive thoughts that feel alien to who you are, do you perform specific physical or mental rituals in response to them, and does the relief from those rituals last only minutes before the doubt returns? If this obsession-compulsion-relief-return cycle is present, OCD may be a more accurate description of your experience than generalised anxiety. A clinical assessment with an OCD-specialist is the right next step.
Can anxiety treatment make OCD worse?
Yes. Some standard anxiety treatment approaches can maintain or strengthen the OCD cycle. Reassurance-seeking in OCD is a compulsion, so providing reassurance maintains the cycle rather than breaking it. Relaxation techniques used to manage the anxiety produced by an intrusive thought can become compulsions themselves. Cognitive restructuring that attempts to challenge or neutralise the intrusive thought can function as a mental compulsion. None of these approaches interrupt the obsession-compulsion cycle, which is what ERP is specifically designed to do.
Why did my doctor not identify it as OCD?
OCD is one of the most underdiagnosed conditions in India. The primary reasons are that OCD shares surface features with anxiety, that people with OCD often do not disclose the specific content of their intrusive thoughts or their compulsions due to shame, and that many clinicians outside specialist settings have limited specific training in OCD diagnosis. This is a systemic problem rather than a failure by any individual clinician or patient.
What is the right treatment for OCD?
Exposure and Response Prevention therapy, known as ERP, is the gold-standard treatment for OCD. It works by deliberately exposing the person to their obsessive trigger and preventing the compulsive response. This breaks the reinforcement cycle by teaching the brain that the feared outcome does not require a compulsion to manage. Medication, particularly SSRIs, is also evidence-based for OCD and is often used alongside ERP for moderate to severe presentations. Medication decisions should always be made in consultation with a psychiatrist who has OCD experience.
Is OCD just a form of anxiety?
OCD was historically classified within the anxiety disorders but was reclassified in the DSM-5 in 2013 into its own category: Obsessive-Compulsive and Related Disorders. This reflects clinical evidence that OCD's defining feature is the obsession-compulsion cycle, not anxiety itself. Anxiety is a prominent symptom of OCD, but the mechanism and the optimal treatment are distinct from anxiety disorders. Understanding OCD as its own condition defined by the compulsion cycle is important for accessing the right treatment.
Does OCD go away on its own?
OCD tends not to resolve without treatment. Left untreated, OCD typically maintains its severity or worsens over time as compulsions become more elaborate and avoidance expands. However OCD is highly treatable with ERP. Most people who engage with ERP therapy see significant and lasting reduction in symptoms. The goal is not to eliminate intrusive thoughts, which is not possible and not the right aim, but to reach a point where the compulsion cycle is broken and the thoughts no longer drive behaviour.
Sources
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). American Psychiatric Publishing; 2022. psychiatry.org/psychiatrists/practice/dsm
Abramowitz JS, Taylor S, McKay D. Obsessive-compulsive disorder. The Lancet. 2009;374(9688):491-499. pubmed.ncbi.nlm.nih.gov/19665647
Salkovskis PM. Obsessional-compulsive problems: a cognitive-behavioural analysis. Behaviour Research and Therapy. 1985;23(5):571-583. pubmed.ncbi.nlm.nih.gov/4051930
Janardhan Reddy YC, Rao NP, Khanna S. An overview of Indian research in obsessive compulsive disorder. Indian Journal of Psychiatry. 2010;52(Suppl 1):S200-S209. pmc.ncbi.nlm.nih.gov/articles/PMC3146215
National Institute of Mental Health. Obsessive-Compulsive Disorder. nimh.nih.gov/health/topics/obsessive-compulsive-disorder-ocd
International OCD Foundation. About OCD. iocdf.org/about-ocd