
Intrusive Sexual Thoughts and OCD: What They Mean and What They Don't
Written by Armaan Raheja, Founder of breakOCD | Clinically reviewed by Dr. Sachi Pandya, Psychologist, Mumbai
This article is for you.
Not to reassure you that everything is fine. Not to tell you what you want to hear. But to explain, clearly and honestly, what is actually happening, because understanding it is the first step to not being controlled by it.
Intrusive sexual thoughts are one of the most common presentations of OCD. They are also one of the least talked about, in India especially, where sexuality carries enormous social and cultural weight, and where shame can keep people silent for years. Many people reading this have never told a single person about these thoughts. Some have been carrying them alone for a decade or more.
That ends here.
What Intrusive Sexual Thoughts in OCD Actually Are
Intrusive thoughts, meaning unwanted and distressing thoughts that arrive uninvited, are a universal human experience. Research consistently shows that most people, at some point, have thoughts involving sexual content that they did not choose and would not want. The thought arrives, it feels strange or wrong, and for most people it passes without much significance.
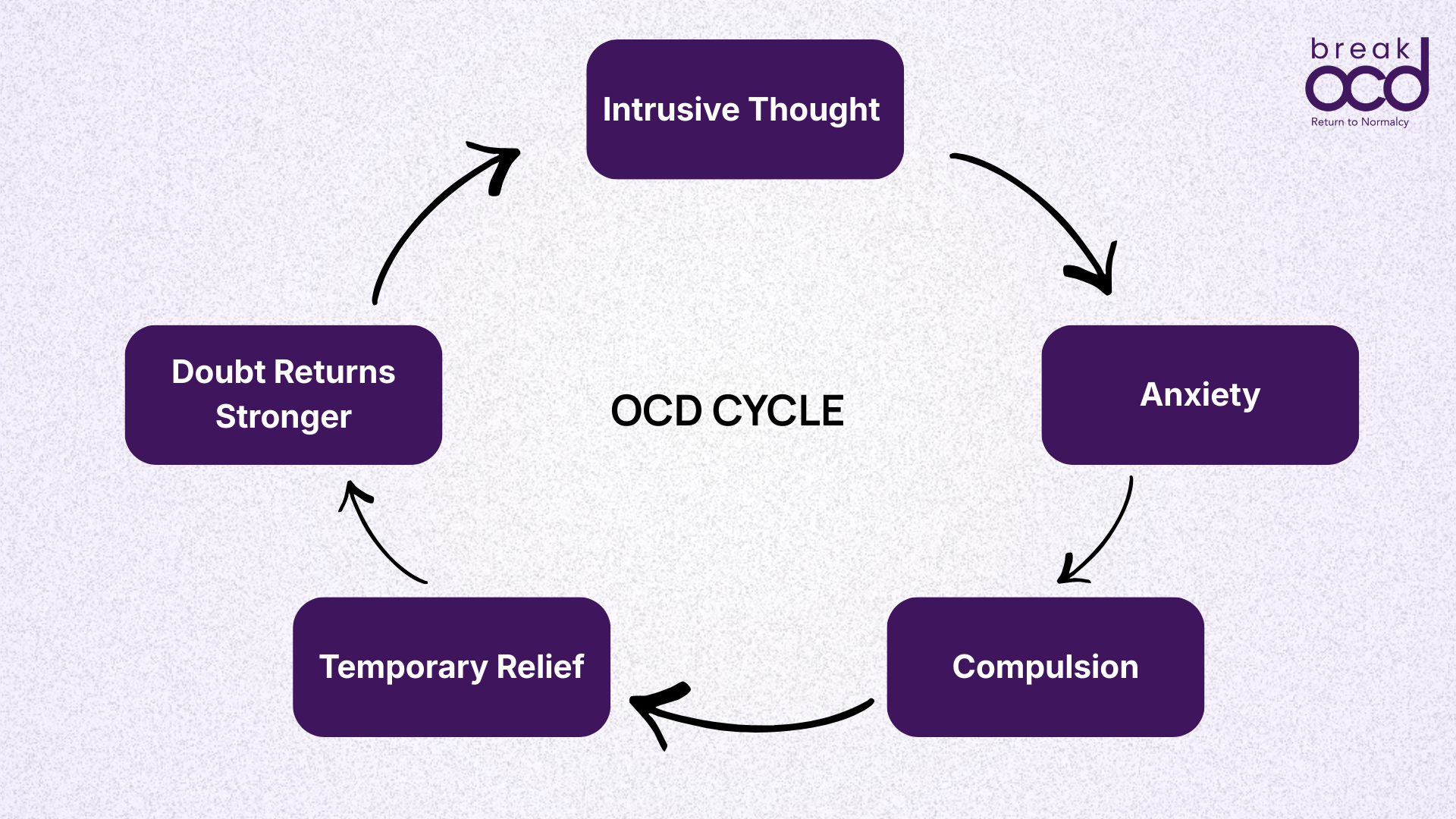
For someone with OCD, the thought does not pass. It gets caught. The brain flags it as deeply significant, treats it as a threat, and demands a response. The person begins asking: why did I have that thought? What does it mean? Does it say something about who I am? Could I act on it?
The harder they try to answer those questions, the louder the thought becomes. The louder the thought becomes, the more certain it feels that it must mean something. This is the OCD cycle, and intrusive sexual thoughts follow exactly the same mechanism as every other OCD presentation.
There is a specific term in psychiatry for why these thoughts feel so foreign and so wrong. The clinical term for this is ego-dystonic. The thought is completely alien to the person's values, identity, and sense of self. It does not feel like them. It does not reflect what they desire. It horrifies them.
That horror is not incidental. It is the most clinically important signal in this entire presentation. People who actually want to act on a sexual thought are not horrified by it. The very fact that the thought causes distress, shame, and desperate attempts to make it stop is evidence that it is ego-dystonic, meaning it goes against everything you are.
The Different Presentations: What This Looks Like
Intrusive sexual thoughts in OCD come in many forms. What they share is the ego-dystonic quality. The thought is not desired, not pleasurable, and not aligned with who the person is. Here are the presentations that appear most commonly in clinical practice.
Intrusive thoughts involving children (POCD)
One of the most distressing presentations of sexual OCD involves intrusive thoughts about children. The person may have a sudden, unwanted thought or image involving a child and feel immediate, overwhelming horror. They may avoid children entirely, stopping themselves from holding a baby, volunteering at a school, or being alone with a niece or nephew, because the thought feels like evidence of something dangerous.
It is not. Research is unambiguous on this point: there are no recorded cases of a person with OCD acting on their obsessions. The horror, the avoidance, the desperate attempts to suppress the thought. All of these are the signature of OCD, not of genuine predatory intent. A person who is genuinely attracted to children does not spend their days terrified of the thought and searching for reassurance that they are safe to be around children.
Intrusive thoughts involving family members
Incest-themed intrusive thoughts are another common presentation that carries enormous shame, particularly in India where family relationships are deeply sacred. The thought may involve a parent, sibling, or other family member. It arrives uninvited, feels completely wrong, and produces immediate guilt and distress.
In Indian families, where physical closeness between family members is normal and expected, these thoughts can make ordinary family interactions feel terrifying. The person may begin creating distance from people they love, inventing reasons to avoid being alone with them, or monitoring every interaction for signs that the thought might be true.
None of this reflects genuine desire. It reflects OCD attaching itself to the most important relationships in a person's life, which is exactly what OCD does.
Sexual orientation OCD (SO-OCD)
Sexual orientation OCD involves intrusive doubts about one's sexual orientation. A heterosexual person may have recurring thoughts asking whether they are actually gay. A gay or bisexual person may have thoughts questioning whether their identity is real. The thoughts create relentless uncertainty that cannot be resolved no matter how much evidence the person examines.
This presentation is frequently misunderstood, including by therapists who are not familiar with OCD. The thoughts are not a sign of repressed identity. They are a sign of OCD attacking something the person values and is certain about. The doubt itself, the inability to feel sure, is the symptom, not the content of the thought.
In India, where homosexuality carries significant social stigma in many communities, SO-OCD can be particularly isolating. A heterosexual person with SO-OCD may be terrified to seek help because they fear being told they are gay. A gay person with SO-OCD may fear the thoughts are telling them their identity is not real. Both presentations are OCD. Both respond to ERP.
Unwanted sexual thoughts during intimacy
Some people experience intrusive sexual thoughts specifically during moments of intimacy with a partner, things like thoughts about someone else, something taboo, or a situation that feels completely wrong. The thought arrives at the worst possible moment and produces immediate shame, guilt, and anxiety.
This can significantly impact relationships and sexual intimacy. The person may begin avoiding sex to avoid the thought. Or they may engage in mental rituals during intimacy, trying to suppress the thought, mentally reviewing whether they genuinely desired the experience, or seeking reassurance from their partner in ways that feel impossible to explain.
Intrusive thoughts about strangers or public situations
Intrusive sexual thoughts can also involve strangers, people the person barely knows, or inappropriate public situations. The person may have a sudden thought in a crowded place and feel immediate horror, followed by obsessive checking of whether the thought means something, avoidance of that location, or prolonged mental reviewing of the experience.
The Groinal Response: The Most Misunderstood Part
There is one aspect of sexual OCD that people almost never talk about, and which causes some of the deepest suffering. It is called the groinal response.
Approximately 40% of people with sexual intrusive thoughts in OCD report experiencing a physical sensation in the genital area when the intrusive thought arrives. This sensation is not sexual arousal in the way most people understand it. It is the body's anxiety response, the same fight-or-flight system that makes your heart pound and your palms sweat, manifesting in a part of the body that feels profoundly significant given the content of the thought.
For the person experiencing it, the groinal response feels like confirmation of their worst fear. If my body responded, doesn't that mean part of me wanted it? The answer is no. And understanding why is one of the most important things a person with sexual OCD can learn.
When the brain flags something as dangerous and fires the anxiety alarm, the body responds. The more the person checks whether the response is there: monitoring their body, testing themselves in triggering situations, mentally examining whether they felt something. The more heightened the awareness becomes, and the more the normal, involuntary sensations are amplified.
Checking for the groinal response is itself a compulsion. It creates the very thing the person is most afraid of. The only answer is to stop checking entirely. Which is exactly what ERP addresses.(delaying compulsion,less and less response to the compulsion, sitting with the discomfort till the anxiety passes, gradually stopping it entirely)
The Compulsions: What People Do With These Thoughts
The compulsions that develop around intrusive sexual thoughts are often invisible to everyone else. They happen entirely inside the mind or in small, private behaviours that no one around the person can see. This invisibility is part of why so many people go undiagnosed for years.
Common compulsions in sexual OCD include:
Mental reviewing: replaying the thought or the situation over and over, trying to determine whether genuine desire was present or whether the thought means something specific about character
Body checking: monitoring physical sensations during or after the thought, testing for the groinal response, body scanning to assess whether genuine arousal is present
Googling: searching for information about what intrusive sexual thoughts mean, whether they indicate something about identity or intent, reading forums and websites for reassurance
Avoidance: staying away from children, family members, certain locations, or intimate situations to prevent the thought from arising
Confession: telling a partner, friend, or family member about the thought in an attempt to feel reassured that they are not judged
Reassurance-seeking: asking questions indirectly or directly to get confirmation that the thought is not meaningful or dangerous
Suppression: using mental force to push the thought away, replacing it with a 'good' thought, praying the thought away, mentally neutralising it
Testing: deliberately exposing themselves to triggering situations to see how they respond, then interpreting the response as evidence
Every single one of these compulsions, though they feel necessary in the moment, makes the OCD cycle stronger. Each compulsion tells the brain: this thought is worth responding to. Which ensures the thought returns.
Why This Is Especially Hard in India
Intrusive sexual thoughts are difficult to carry anywhere. In India, they carry additional weight that makes them particularly isolating.
Sexuality is rarely discussed openly in Indian families or communities. Most people have received no framework for thinking about sexual thoughts, wanted or unwanted, as a normal part of human experience. When an intrusive sexual thought arrives, particularly one involving a family member or a child or same-gender content, there is no cultural script that helps the person understand it. There is only shame.
The shame in India carries specific dimensions. For a person from a deeply religious background, an intrusive sexual thought during prayer, about a religious figure, or involving a family member can feel like a catastrophic moral and spiritual failure. For a person in an arranged marriage, intrusive doubts about sexual attraction to their spouse can feel like a threat to the entire foundation of family life. For a person whose community holds strong views on homosexuality, SO-OCD thoughts can feel too dangerous to acknowledge even privately.
These layers of cultural shame are not incidental to the OCD. They are part of why the OCD is so loud. OCD attacks what matters most. In India, sexuality, family, faith, and moral character matter enormously. Which is exactly why OCD goes there.
Many people in India have been carrying intrusive sexual thoughts for five, ten, or twenty years without telling anyone, including their doctors. Some have been misdiagnosed with depression or general anxiety. Some have been told to pray harder. Some have been told they are morally deficient. None of these responses are correct. And all of them delay access to treatment that actually works.
What These Thoughts Do Not Mean
Because this needs to be stated clearly and without qualification:
Having an intrusive sexual thought about a child does not mean you are attracted to children.
Having an intrusive thought about a family member does not mean you desire them.
Having intrusive thoughts that question your sexual orientation does not mean your identity is different from what you know it to be.
Experiencing a groinal response during an intrusive thought does not mean the thought reflects genuine desire.
Having these thoughts repeatedly does not make them more true or more dangerous with each repetition.
Being unable to suppress the thought does not mean you want it there.
There are no recorded cases of a person with OCD acting on their obsessions. The literature on this is consistent and unambiguous. The distress, the avoidance, the desperate attempts to neutralise the thought. These are the signature of OCD. They are incompatible with genuine intent.
A thought is not a desire. A thought is not a plan. A thought is not who you are.
Treatment: What Actually Works
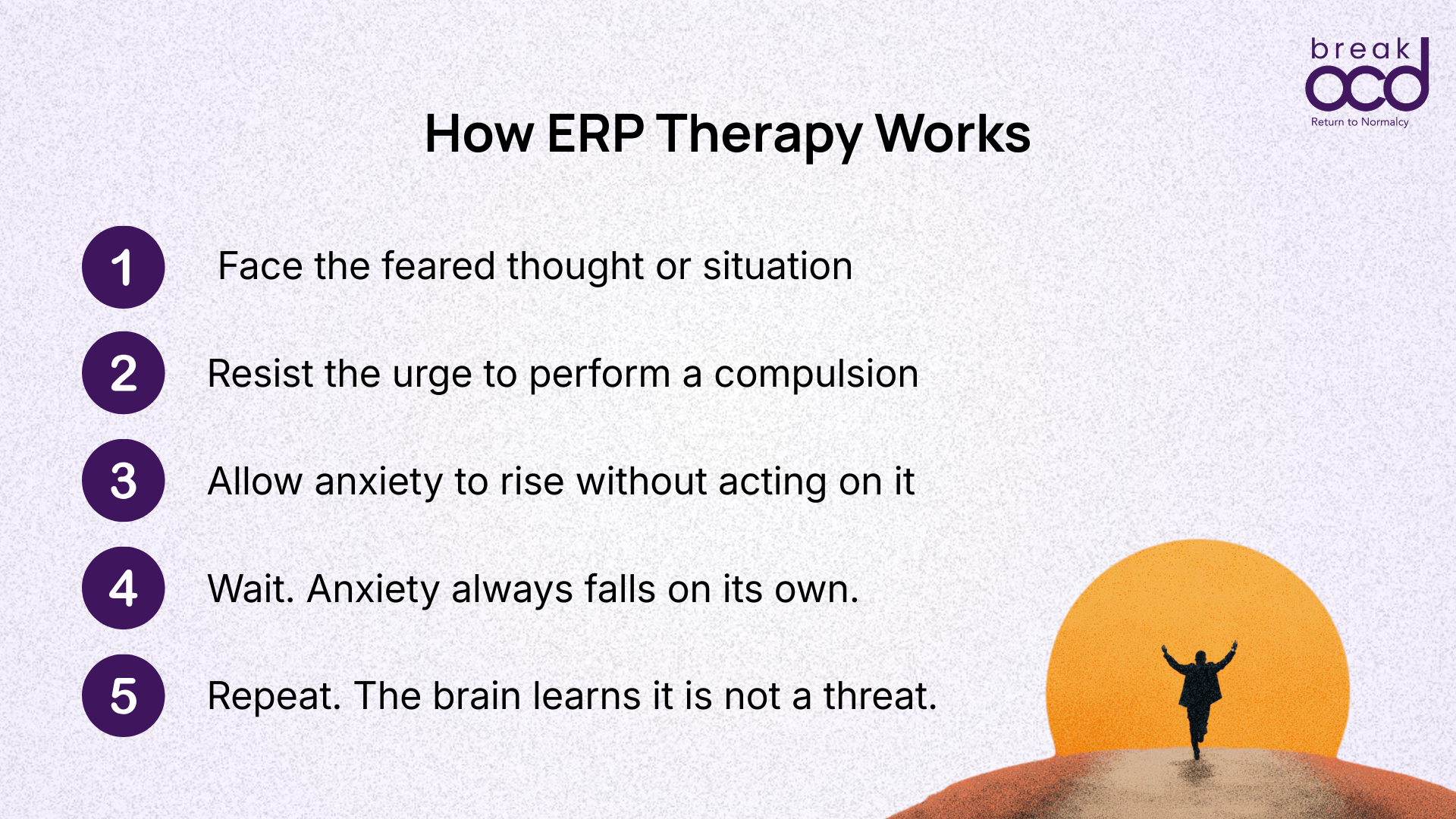
Sexual OCD responds to the same treatment as every other OCD presentation, Exposure and Response Prevention therapy, or ERP. The principles are identical, though the specific application differs based on the nature of the intrusive thoughts and the compulsions that have developed around them.
ERP for sexual OCD typically involves:
Imaginal exposures: deliberately bringing the feared thought to mind and sitting with it without engaging in any compulsion in response. Not suppressing it. Not analysing it. Allowing it to exist without treating it as a signal that requires action.
Response prevention for mental compulsions: specifically stopping the reviewing, the checking, the reassurance-seeking, the googling, and the body monitoring that maintain the cycle.
Behavioural exposures: gradually reintroducing avoided situations. Being near children again. Sitting with a family member without monitoring thoughts. Engaging in intimacy without mentally reviewing the experience afterwards.
Stopping the groinal check: one of the most important and most difficult response prevention targets in this presentation. Each time the urge to check for the groinal response arises, response prevention means not checking.
ERP for sexual OCD requires working with a therapist who specifically understands OCD and this presentation. General therapy, including general CBT, is not sufficient and can make things worse by engaging with the content of the thoughts rather than the cycle that sustains them. A therapist who treats OCD will not be alarmed by the content of the thoughts. They will have heard them before, across hundreds of patients.
In many cases, medication, specifically SSRIs, is used alongside ERP for moderate to severe presentations. Medication reduces the intensity of the intrusive thoughts and lowers baseline anxiety to a level where ERP becomes more accessible. The decision about whether medication is appropriate is one to make with a psychiatrist who understands OCD.
On Seeking Help
Many people with sexual OCD are afraid to seek help because they fear that disclosing the content of their thoughts will result in judgment, legal consequences, or confirmation of their worst fear about themselves.
A qualified mental health professional who understands OCD will not judge you for the content of your thoughts. They will not report you to anyone. They will not treat your distress as evidence of genuine intent. They have sat with hundreds of people who have told them the same things you have been carrying alone.
The most important thing you can do is find a professional who specifically understands OCD, not general anxiety and not general CBT. Ask directly: have you worked with intrusive sexual thoughts in OCD before? A specialist who has, will answer that question without hesitation.
You do not have to carry this alone. And you do not have to keep suffering simply because no one has given you a language for what you are experiencing.
Frequently Asked Questions
Does having intrusive sexual thoughts mean I want to act on them?
No. Intrusive sexual thoughts in OCD are ego-dystonic: they are completely contrary to your values and desires. The distress and horror you feel about the thought is the clearest evidence that it does not reflect genuine intent. There are no recorded cases of a person with OCD acting on their obsessions.
What is the groinal response and does it mean I am genuinely aroused?
The groinal response is an involuntary physical sensation in the genital area that can occur during intrusive sexual thoughts. It is driven by anxiety, not genuine sexual desire. Physical arousal and psychological desire are not the same thing: a well-documented phenomenon called arousal non-concordance. The groinal response is a symptom of OCD, not evidence of desire.
I have been having these thoughts for years. Does that mean they are true?
No. The persistence of intrusive thoughts in OCD has nothing to do with their truth or significance. OCD thoughts persist because of the cycle that maintains them: the anxiety, the compulsions, the attempts to resolve the doubt. Longer duration reflects the strength of the cycle, not the validity of the thought.
Can I tell a therapist about these thoughts without facing consequences?
Yes. A therapist's confidentiality obligations apply to intrusive sexual thoughts. Intrusive thoughts are not the same as genuine intent, and a qualified mental health professional understands this distinction clearly. The only exceptions to confidentiality involve genuine, credible, imminent risk: which OCD intrusive thoughts, by their nature, do not represent.
Is sexual OCD treatable?
Yes, highly so. ERP is effective for all presentations of sexual OCD including POCD, SO-OCD, incest-themed thoughts, and unwanted thoughts during intimacy. The treatment follows the same principles as ERP for any other OCD presentation. Many people who have carried these thoughts alone for years experience significant and sustained improvement with proper treatment.
I am in India and afraid no one will understand. What should I do?
Finding a therapist who specifically understands OCD: not just general anxiety: is the most important step. Ask directly whether they have experience with intrusive sexual thoughts in OCD. A specialist who has worked with this presentation will not be alarmed, will not judge you, and will have heard similar disclosures many times before. breakOCD's clinical panel includes specialists with specific OCD expertise.
Sources
International OCD Foundation: Unwanted Intrusive Thoughts
Cambridge Core: Risk assessment and management in obsessive-compulsive disorder — Advances in Psychiatric Treatment
PubMed Central: Psychodynamic Perspective of Sexual Obsessions in OCD — Chaudhary S, Singh AP, Varshney A
PubMed Central: An overview of Indian research in obsessive compulsive disorder — Reddy, Rao, Khanna
NCBI StatPearls: Obsessive-Compulsive Disorder
Neurolaunch: Understanding Groinal Response: Navigating OCD and Arousal Non-Concordance