
What Does OCD Feel Like?
The internal experience of OCD, and why it is so hard to explain to someone who has never had it.
Written by Armaan Raheja, Founder of breakOCD | Clinically reviewed by Dr. Shorouq Motwani, Psychiatrist, Mumbai
In This Article
- OCD Does Not Look the Way Most People Think
- What OCD Actually Feels Like
- Why OCD Thoughts Feel So Personal
- The Emotional Weight of Living with OCD
- What OCD Feels Like in an Indian Context
- The Difference Between OCD and Ordinary Worry
- OCD Is a Disability, Not a Quirk
- There Is a Way Through
- Frequently Asked Questions
OCD is one of the most misunderstood mental health conditions in the world. Most people think they know what it looks like. Most people are wrong.
If you live with OCD, you have probably struggled to explain it to someone. The words never quite capture it. You might say you get anxious, or that you overthink, or that certain thoughts bother you. But none of that fully describes what it actually feels like to be inside your own mind when OCD is running.
OCD is recognized as one of the most disabling psychiatric conditions in the world. In India, where the lifetime prevalence is estimated at 2 to 3 percent of the general population, millions of people are living with it right now, many of them without a name for what they are experiencing.
This article is for them. And for anyone who loves them and wants to understand.
OCD Does Not Look the Way Most People Think
Ask someone on the street what OCD looks like and they will describe a person who washes their hands repeatedly or arranges objects in neat rows. These are real experiences for some people with OCD. But they represent only a fraction of the full picture.
Many people with OCD have no visible rituals at all. Their compulsions happen entirely inside the mind. From the outside, they look completely fine. Internally, they are exhausted.
Others have rituals that look ordinary, like re-reading a message before sending it, checking a lock twice, or asking for reassurance from a loved one. These behaviors seem reasonable in isolation. It is only when you understand the anxiety driving them, and how little relief they actually provide, that the pattern becomes clear.
OCD is not a personality trait. It is not being particular, or detail-oriented, or cautious. It is a mental health condition driven by a misfiring threat system in the brain, and it feels very different from those things.
What OCD Actually Feels Like
The most honest way to describe OCD is this: it feels like being afraid of your own mind.
Not afraid of external things, like spiders or heights, where the threat is outside of you. Afraid of your own thoughts. Afraid of what they might mean. Afraid of what you might do, or what might happen, or who you might really be.
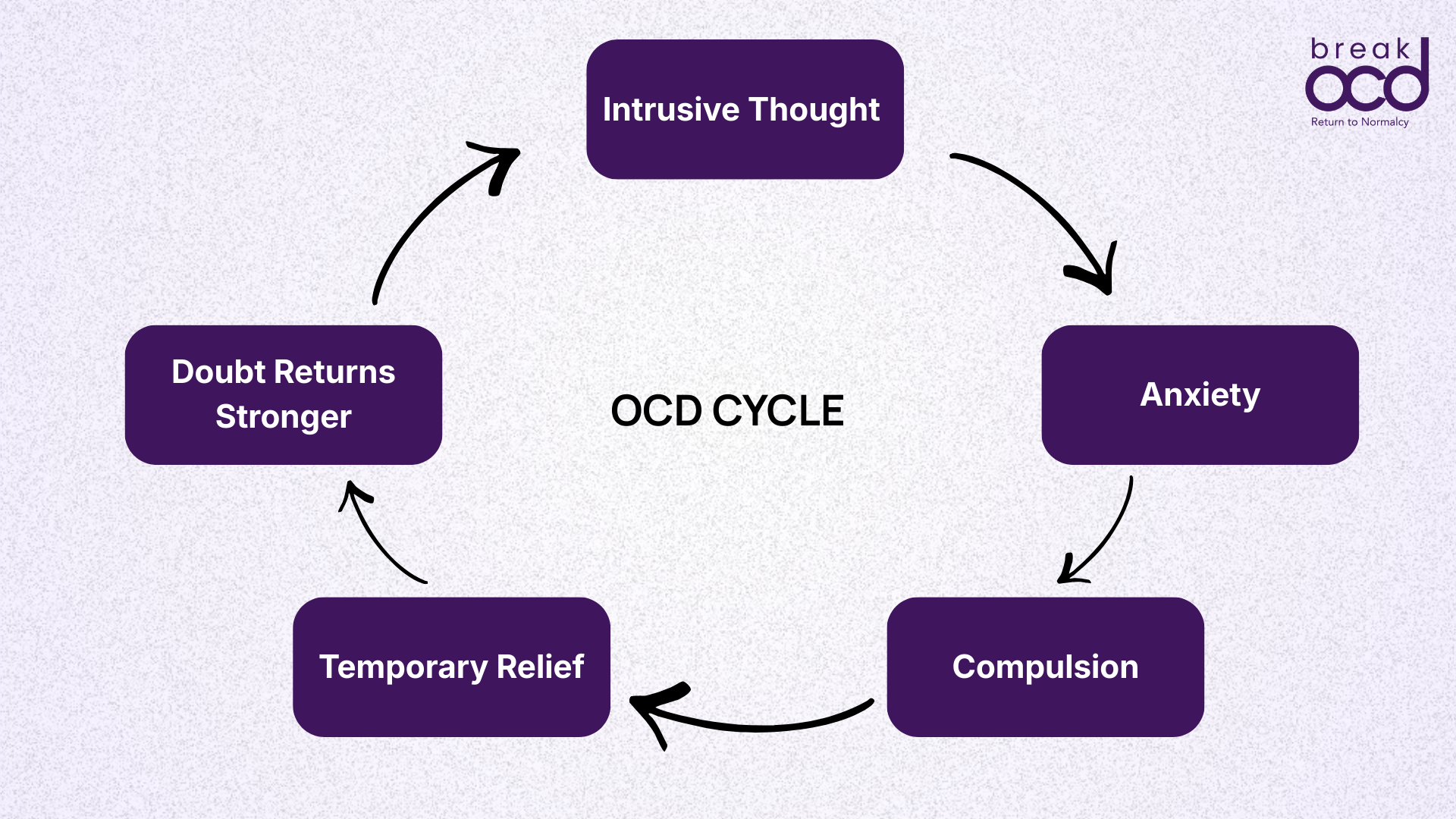
People with OCD commonly describe:
A thought arriving that feels deeply wrong or dangerous
An immediate surge of anxiety, dread, or what many describe as a sense of impending doom
A powerful urge to do something, anything, to make that feeling go away
Temporary relief when the compulsion is performed
The thought returning, often stronger than before
The whole cycle starts again
What makes this so exhausting is that it never fully stops. The mind is constantly monitoring itself, scanning for threats, flagging thoughts as dangerous. For someone with OCD, the brain cannot tell the difference between a genuine threat and a random intrusive thought. Both get the same alarm.
Many people with OCD describe it as having a bully living inside their head. One who knows exactly what frightens you most, and goes there every time.
Why OCD Thoughts Feel So Personal
One of the most distressing things about OCD is that the intrusive thoughts feel deeply personal, even though they are not chosen.
OCD does not latch on to things that do not matter to you. It targets what you care about most. If being a good person matters deeply to you, OCD will fill your mind with thoughts that question your morality. If your faith is central to your life, religious OCD will attack your relationship with God. If you love your family more than anything, the thoughts will involve harm coming to them.
This is not a coincidence and it is not a sign of who you are. It is how OCD works. The more something matters, the more emotionally charged an intrusive thought about it becomes, and the harder it is to dismiss.
The result is that people with OCD often carry enormous shame. They believe their thoughts reveal something terrible about their character. They hide them. They carry them alone.
The clinical term for this is ego-dystonic, meaning the thoughts go sharply against the person's own values and sense of self. This is one of the key differences between OCD and something like a genuine urge or desire. OCD thoughts horrify the person having them. That horror is not a coincidence. It is the whole mechanism.
The Emotional Weight of Living with OCD
OCD is not just a thought disorder. It is an emotional experience that affects every part of a person's life.
Exhaustion
Living with OCD is mentally exhausting in a way that is difficult to convey. The constant internal monitoring, the cycles of anxiety and compulsion, the mental rituals that can go on for hours quietly inside the mind. People with OCD often describe feeling drained by lunchtime on an ordinary day, having spent the morning managing thoughts that no one else could see.
Shame
Because OCD tends to target taboo areas, including harm, sexuality, religion, and morality, many people feel profound shame about their thoughts. In India, where these subjects carry additional cultural and social weight, the shame can be particularly isolating. Many people with OCD go years without telling a single person what is happening in their mind.
Doubt
OCD has been called the doubting disease, and that name fits. Not general indecisiveness, but a very specific kind of doubt that never resolves. The person knows logically that everything is probably fine. But they cannot feel it. The gap between knowing and feeling is where OCD lives.
Frustration
Perhaps the most frustrating part of OCD for many people is that they are completely aware their fears are irrational, and yet that awareness does nothing to reduce the anxiety. You can know with absolute certainty that a thought is not true and still feel the dread of it as if it were. This leads many people to feel like they are failing somehow, that they should be able to think their way out of it. This is not a failure. It is simply how OCD works.
Isolation
Because so much of OCD happens internally, it is an invisible condition. A person can be sitting in a room full of people, appearing calm, while internally managing a loop of intrusive thoughts and compulsions that has been running for hours. This invisibility makes it deeply isolating. The people around them have no idea. And because the thoughts often feel too strange or too shameful to share, the person rarely tells them.
What OCD Feels Like in an Indian Context
In India, the experience of OCD carries additional layers that are worth naming directly.
Family is central to Indian life, and OCD frequently targets family relationships. Intrusive thoughts could center around harming a parent, sibling, or child are common and cause immense distress. So is relationship OCD, which involves relentless doubt about whether you truly love your partner, a particularly painful experience in the context of arranged marriages where the stakes feel very high.
Religious OCD is extremely prevalent in India, given the deep importance of faith across communities. Blasphemous intrusive thoughts, fear of offending God, and compulsive praying or ritual repetition are among the most common forms of OCD seen in Indian clinical settings. For many people, these thoughts feel like the most unacceptable thing they can imagine, which is exactly why OCD fixates on them.
Shame around mental health in India means that many people with OCD interpret their experience through a moral or spiritual lens rather than a clinical one. They believe they are bad people, or that they are being tested by God, or that their thoughts reflect hidden desires. None of these interpretations are accurate, and all of them delay the person getting the right help.
The average time between OCD onset and correct diagnosis is estimated at seven years globally. In India, that gap is likely longer. Many people are misdiagnosed with general anxiety or depression first. Some receive no diagnosis at all.
You are not your thoughts. In OCD, the thoughts that cause the most distress are usually the ones that conflict most sharply with who you actually are.
The Difference Between OCD and Ordinary Worry
Everyone worries. Everyone has intrusive thoughts from time to time. So what makes OCD different?
The difference lies in what happens next.
For most people, an uncomfortable thought passes. It might be noted briefly, found strange or unsettling, and then the mind moves on. The thought does not demand a response.
For someone with OCD, the thought does not pass. It gets caught. The mind treats it as a genuine signal of danger and begins demanding a response. The person must analyze it, neutralize it, seek certainty about it, or perform some behavior to make the anxiety go away. Until they do, the discomfort is overwhelming.
And even when they do, the relief does not last. The thought, or a version of it, comes back. Each compulsion teaches the brain that the thought was worth responding to, which makes the next intrusion feel even more urgent.
This is the loop. Not thinking too much. Not being anxious. A specific neurological cycle that feeds itself and grows stronger over time without the right treatment.
OCD Is a Disability, Not a Quirk
OCD is recognized as a disability under India's Rights of Persons with Disabilities Act, 2016. This is not a technicality. It reflects the real and serious impact OCD has on a person's ability to work, study, maintain relationships, and live their daily life.
The casual use of OCD as a descriptor for tidiness or perfectionism, 'I am so OCD about my desk,' does genuine harm. It makes it harder for people with the actual condition to be taken seriously. It creates a cultural context in which someone describing their real suffering is met with a smile rather than understanding.
OCD at its most severe is completely debilitating. People lose jobs, relationships, years of their lives to this condition. Even at moderate severity, the daily burden is significant and invisible to almost everyone around the person carrying it.
There Is a Way Through
OCD is one of the most well-researched mental health conditions in the world. The gold-standard treatment, Exposure and Response Prevention therapy, has decades of clinical evidence behind it and works by changing the brain's learned response to intrusive thoughts rather than trying to eliminate the thoughts themselves.
Recovery from OCD does not mean never having intrusive thoughts again. Intrusive thoughts are a normal part of being human. Recovery means changing your relationship with those thoughts so that they no longer trigger the cycle, no longer demand a response, no longer control your decisions.
Many people with OCD go on to live full, deeply meaningful lives. The path begins with understanding what you are actually dealing with, and knowing that what you are experiencing has a name, a mechanism, and a treatment.
You are not broken. Your brain learned the wrong response to uncertainty. That can be unlearned.
Frequently Asked Questions
Does OCD always involve visible rituals like hand washing or checking?
No. Many people with OCD have compulsions that are entirely mental and invisible to others. These include replaying events in the mind, mentally seeking reassurance, analyzing intrusive thoughts for meaning, and silently repeating phrases or prayers. Visible physical rituals are only one form of OCD.
Why do OCD thoughts feel so real even when you know they are irrational?
OCD operates in the emotional learning systems of the brain, not the logical ones. This is why knowing something is irrational does not stop the anxiety. The brain's threat detection system misfires, treating a harmless thought as a genuine danger. The emotional response comes first. Logic comes second, and usually cannot override it without the right treatment.
Is it normal to feel ashamed of OCD thoughts?
Yes, and it is one of the most common reasons people delay seeking help. OCD tends to target taboo subjects including harm, sexuality, religion, and morality. The thoughts are ego-dystonic, meaning they go against the person's own values. They cause distress precisely because the person would never want to act on them. Shame about these thoughts is understandable, but the thoughts themselves are a symptom of OCD, not a reflection of character.
Can OCD feel different from person to person?
Yes. OCD attaches itself to what matters most to the individual, which means the content of intrusive thoughts varies enormously. Two people with OCD can have completely different thought content and very different external behaviors while experiencing the same underlying cycle of obsession, anxiety, compulsion, and temporary relief. The theme changes. The mechanism stays the same.
How is OCD treated?
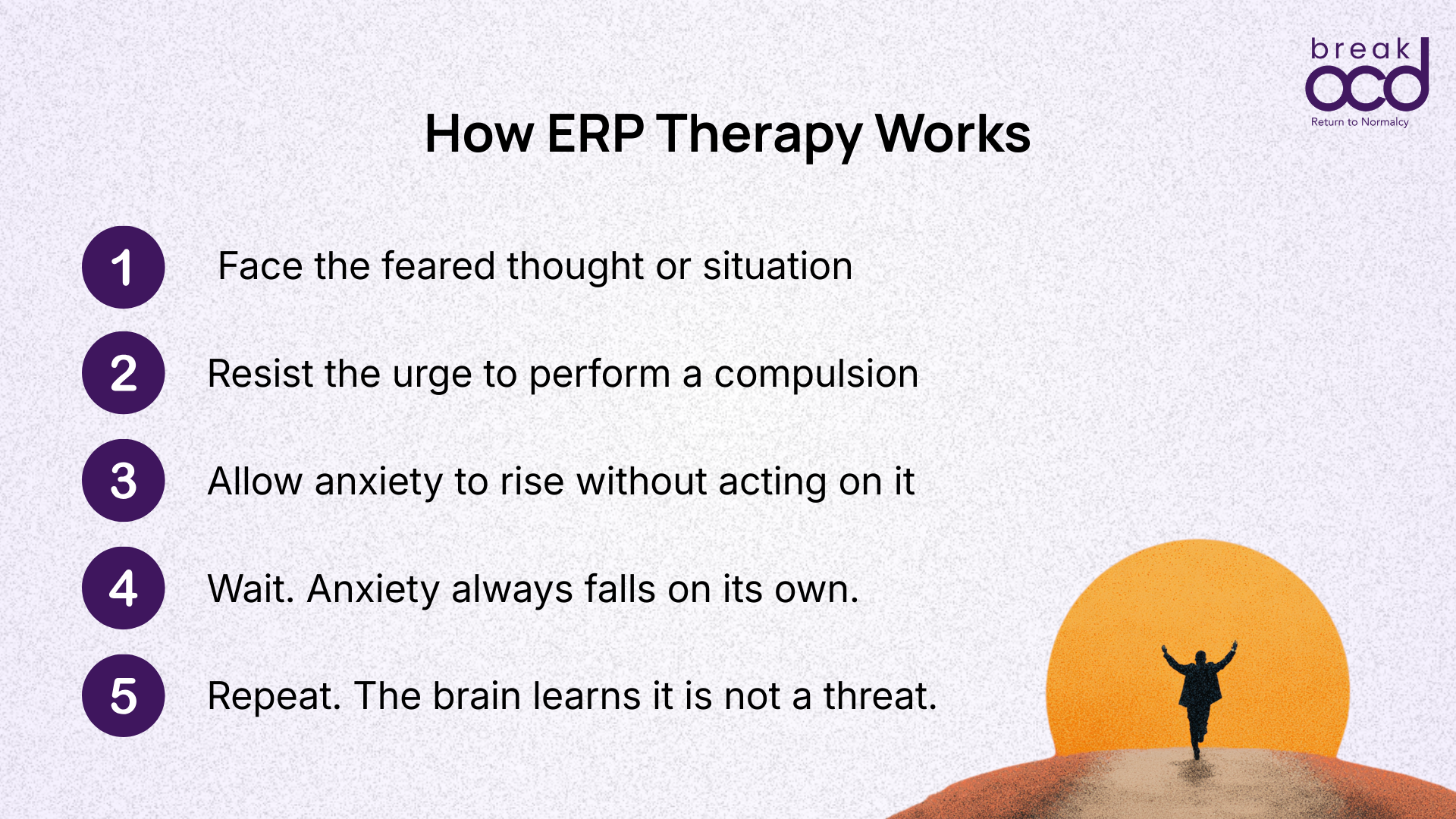
The gold-standard treatment for OCD is Exposure and Response Prevention therapy, or ERP. ERP works by helping people gradually face their feared thoughts and situations without performing compulsions, so the brain learns over time that the thoughts are not dangerous and do not require a response. Medication can also be helpful in some cases. General talk therapy and anxiety treatment alone are typically not sufficient for OCD.
About the Author
Armaan Raheja
Armaan Raheja is the founder of breakOCD, India's first dedicated OCD support app. He was diagnosed with OCD after years of misdiagnosis and went on to study psychology in the United States, where he received evidence-based treatment including ERP therapy. On returning to India and finding a fragmented mental health system with few OCD-specific resources, he built breakOCD to provide the support he wished had existed. Armaan brings both lived experience of OCD and a commitment to evidence-based, stigma-free mental health care in India.
Clinically Reviewed By
Dr. Shorouq Motwani
Dr. Shorouq Motwani is a Psychiatrist at Lilavati Hospital and Research Centre, Mumbai. She specializes in emotional and behavioral disorders, neurodevelopmental disorders, and mental health in adolescents and young adults. She is the recipient of the ASHA Award for best paper presentation and has multiple published research papers in psychiatry.
Sources & Further Reading
NHS: Obsessive Compulsive Disorder Overview
Government of India: Rights of Persons with Disabilities Act 2016