
ERP Therapy for OCD: What It Is and Why It Works
Written by Armaan Raheja, Founder of breakOCD | Clinically reviewed by Dr. Sachi Pandya, Clinical Psychologist, Mumbai
In this article
- Why Regular Therapy Does Not Work for OCD
- A Quick Note on Terms
- What ERP Actually Is
- Why ERP Works: The Brain Science
- What ERP Looks Like in Practice
- ERP Across Different OCD Presentations
- What the Evidence Shows
- What Makes ERP Difficult
- ERP, Medication, and Other Treatments
- The Bottom Line
- Frequently Asked Questions
If that sounds familiar, you are not alone. Most people with OCD spend years in therapy without getting better. Not because therapy does not work for OCD, but because they are almost always in the wrong kind.
ERP is different. This article explains what it is, why it works when nothing else does, and what you actually need to know before you start.
Why Regular Therapy Does Not Work for OCD
Standard talking therapies (including generic CBT, psychodynamic therapy, and counselling) share a common principle: examining, understanding, and reframing your thoughts will reduce their power over you. For depression, generalised anxiety, and many other conditions, this is often true.
For OCD, it creates a problem.
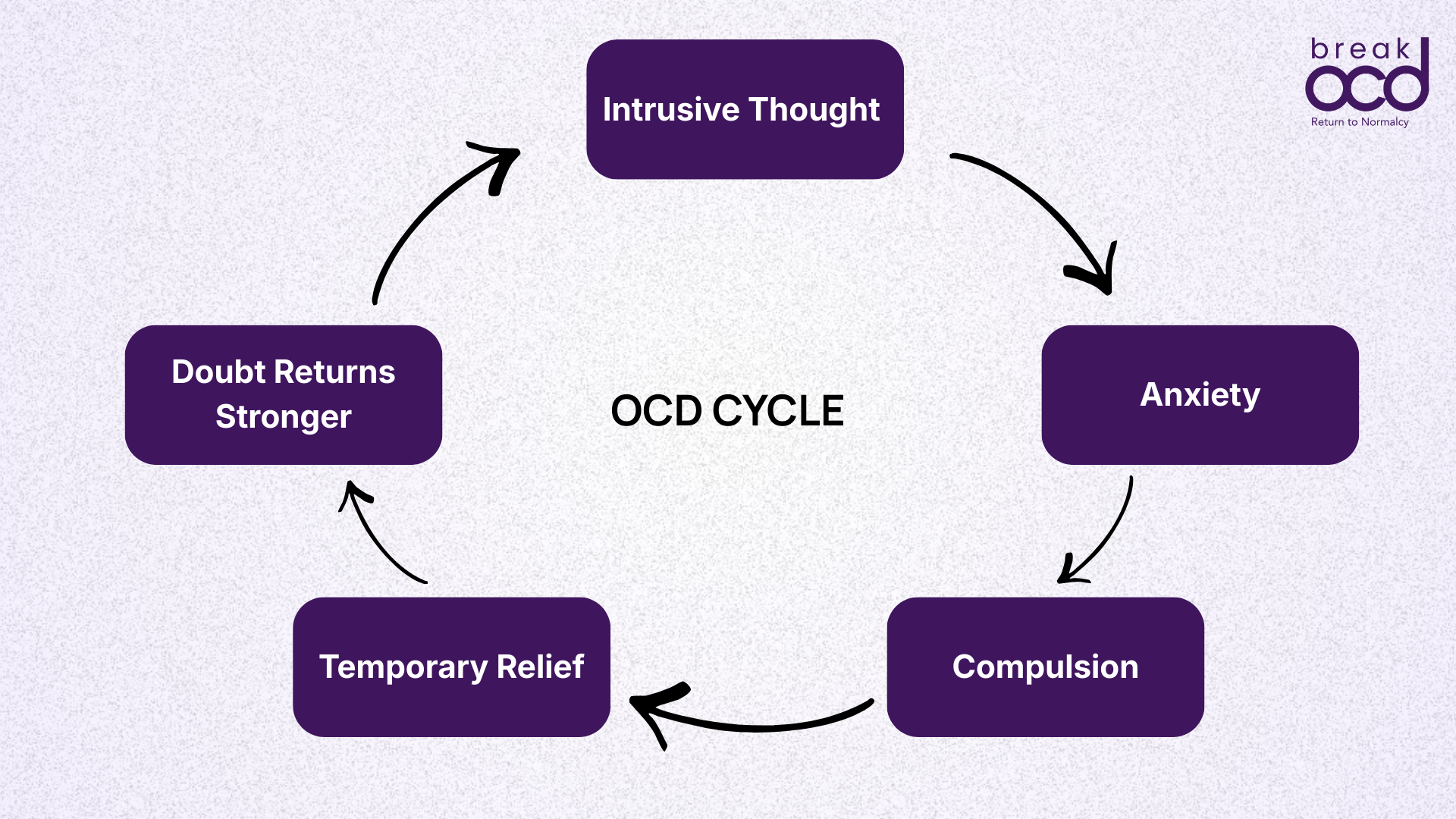
OCD is sustained by a specific cycle. An intrusive thought arrives. You experience anxiety. You perform a compulsion, mental or physical, to reduce that anxiety. The anxiety drops temporarily. The thought returns. With each repetition, the brain's association between the thought and the need to act becomes stronger.
What happens when you spend a therapy session analysing that intrusive thought? You engage with it. You give it attention and significance. You treat it as something that needs to be understood and resolved. This is, functionally, a compulsion. The mental effort to make sense of an OCD thought is often itself maintaining the cycle, not interrupting it.
The International OCD Foundation is direct on this point: there is no research evidence that traditional talk therapy is effective for OCD. A meta-analysis examining randomised controlled trials found ERP more effective than all other therapies and control conditions. The most rigorous comparisons consistently find ERP superior.
It is not that you have not tried hard enough in therapy. It is that standard therapy was not designed for OCD. ERP was.
A Quick Note on Terms
If you are new to OCD, two words come up throughout this article. Here is what they mean:
OCD is the cycle where these two lock together. ERP is the treatment designed to break it.
What ERP Actually Is
ERP stands for Exposure and Response Prevention. Each part describes one of the two things you do in treatment.
Exposure
Exposure means deliberately encountering the thoughts, situations, objects, or sensations that trigger your obsessions. Not avoiding them. Not neutralising them. Encountering them, and staying with the anxiety that follows.
For someone with contamination OCD, this might mean touching a surface they consider dirty without washing their hands afterwards. For someone with harm OCD, it might mean holding a kitchen knife while sitting with a feared thought. For someone whose compulsions are entirely mental, it might mean writing down the thought they most fear, sitting with it on the page, and not engaging in any mental ritual to reduce the discomfort.
The exposures are not random or cruel. They are structured, hierarchical, and collaborative. You and your therapist build a fear hierarchy, a ranked list of exposures from least to most distressing, and work through them gradually, starting where the anxiety is manageable.
Response Prevention
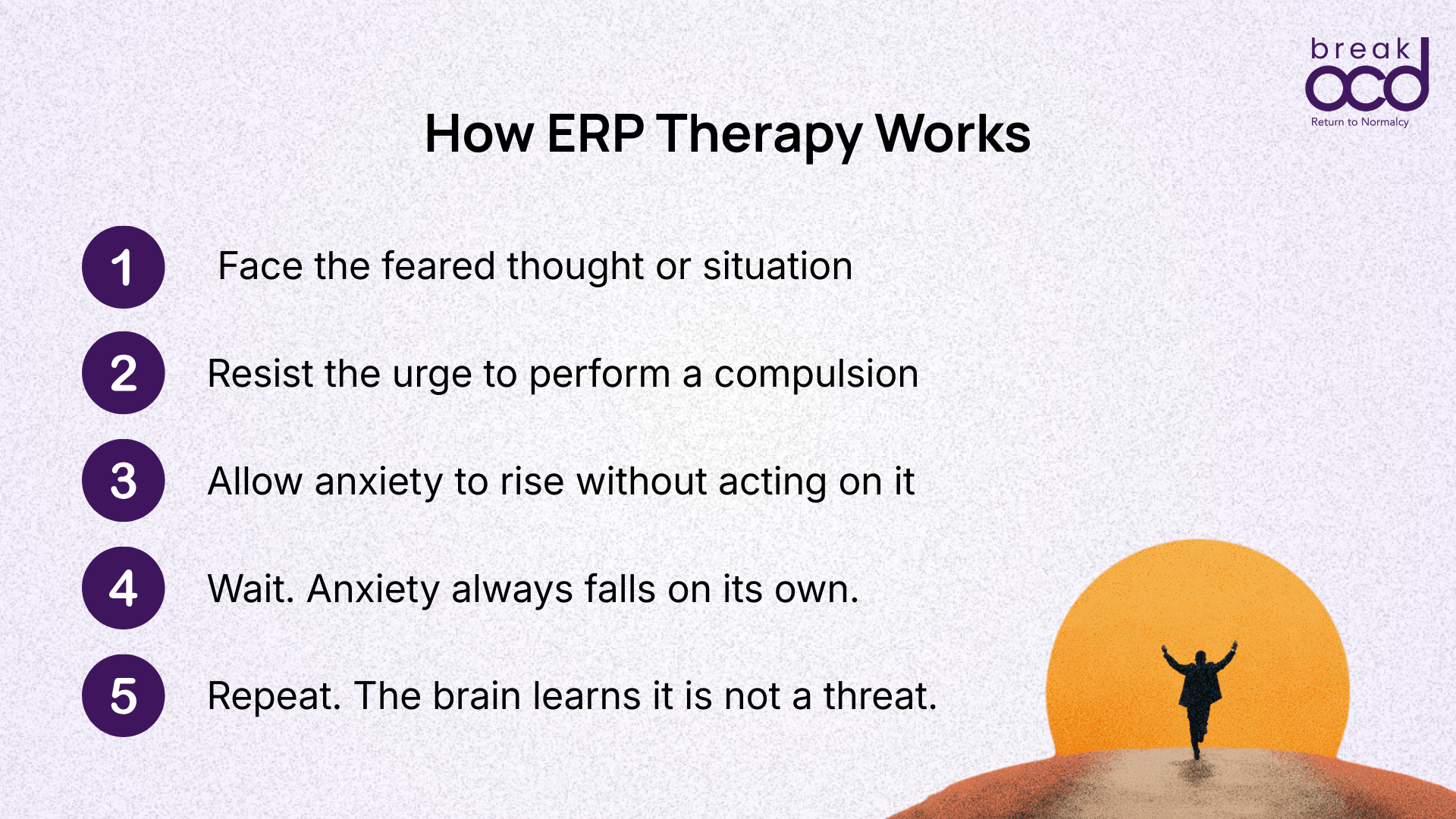
This is the second and equally critical half. After each exposure, you choose not to perform the compulsion.
Not because the urge disappears. It will not, at first. The urge to check, to wash, to seek reassurance, to perform a mental ritual: it will be present and often intense. Response prevention means sitting with that urge without acting on it, for long enough that something important happens.
The anxiety peaks. And then, on its own, it falls.
Not because you resolved the doubt. Not because the feared thing became safe. But because your nervous system begins to recalibrate, learning that the feared outcome did not occur, and that the anxiety itself, though uncomfortable, was not dangerous.
ERP is not about convincing yourself the feared thing is impossible. It is about teaching your brain, through repeated experience, that the anxiety can be tolerated without a compulsion. That is a different thing entirely.
Why ERP Works: The Brain Science
For decades, ERP was explained through habituation theory: repeated exposure to a feared stimulus eventually reduces the anxiety response, and the brain learns through this reduction that the stimulus is not dangerous. This remains partly correct and a useful framework.
Current research has refined this understanding in an important way. The more robust explanation is what researchers call expectancy violation.
The brain does not delete the original fear association. It builds a new, competing one: this situation is not dangerous. In future encounters with the same trigger, the brain can draw on either association. The goal of ERP is to make the non-threatening association strong enough to win.
This is why reassurance-seeking actively undermines recovery. It provides temporary certainty rather than the experience of surviving uncertainty, which prevents the brain from building the new association it needs.
At a neurological level, ERP appears to normalise activity in the brain circuits involved in threat detection and habit formation, circuits that research consistently shows are dysregulated in OCD. ERP is one of the few interventions shown to influence these circuits over time.
OCD feels real because your brain's alarm system is firing at the wrong things. ERP is the process of resetting that alarm. Not by arguing with it, but by outlasting it.
What ERP Looks Like in Practice
ERP is not the same as flooding (the discredited idea of throwing someone straight into their worst fear and waiting for the anxiety to subside). Good ERP is gradual, collaborative, and paced by the person doing it.
Assessment and psychoeducation
In the early sessions, your therapist takes a detailed history: what your specific obsessions are, what compulsions you perform in response, what triggers the cycle most intensely, and what you currently avoid. You also receive psychoeducation: a clear explanation of how OCD works and why each element of ERP matters.
Understanding the rationale for ERP is not just background reading. Research on inhibitory learning suggests that people who understand what they are trying to learn from a specific exposure show better outcomes.
Building the fear hierarchy
Together with your therapist, you build a personalised fear hierarchy: a ranked list of exposures from least to most distressing. Each exposure is specific and concrete. Not 'touch dirty things' but 'touch the outside handle of a public bathroom door and then touch my face.' The specificity matters: vague exposures are easier for the OCD brain to discount.
The hierarchy typically includes 10 to 20 exposures across a range of difficulty. You start at the lower end and build upward as your distress tolerance strengthens.
Conducting exposures
Exposures happen both in-session with your therapist and as homework between sessions. During an exposure, you stay in contact with the feared stimulus until your anxiety subsides or until enough time has passed without a compulsion for the expectancy violation to occur, typically around 45 minutes to an hour in formal sessions.
For mental compulsions and intrusive thoughts, the exposures are imaginal: deliberately bringing the feared thought to mind and sitting with it, without neutralising, analysing, or trying to push it away. This is harder than it sounds, because it requires doing the opposite of everything OCD has been telling you to do for years.
Practice between sessions
The between-session component of ERP is not optional. Research consistently identifies it as one of the strongest predictors of outcome. In daily life, when a compulsion urge arises, you delay or resist it, not because the anxiety is pleasant, but because each time you do, you reinforce the brain's new association.
Delaying a compulsion, even by five minutes at first, is a form of response prevention that begins to interrupt the automatic quality of the OCD cycle.
ERP Across Different OCD Presentations
One of the things that most surprises people is how ERP applies across every type of OCD, including those without any visible physical compulsions.
Contamination OCD
Exposures involve touching feared surfaces, objects, or situations without cleaning or washing afterwards. The hierarchy moves from mild contamination concerns to the ones that feel most threatening. Response prevention means not washing, wiping, or seeking reassurance after the exposure.
Checking OCD
Exposures involve leaving the house without checking the lock, turning off an appliance without going back to verify, sending a message without re-reading it. Response prevention means sitting with the uncertainty that follows, without returning to verify.
Harm OCD
Exposures are often imaginal: deliberately bringing the feared thought to mind, writing it out, being near the objects or situations associated with the fear. Response prevention means not seeking reassurance, not confessing the thought to others, not avoiding the triggering context, and not performing any mental ritual to neutralise the thought.
Relationship OCD (ROCD)
Exposures involve sitting with the uncertainty of not knowing, without resolving the doubt about whether the relationship is right or the feelings are real. Response prevention means not seeking reassurance from a partner, not googling, not mentally comparing, and not analysing the relationship to find certainty.
Religious OCD (Scrupulosity)
Exposures involve sitting with blasphemous intrusive thoughts without mentally praying them away, engaging in religious practices without performing extra rituals to feel 'right,' and tolerating the uncertainty of not knowing whether one has offended God. This is among the most culturally specific presentations in an Indian context, and one of the most common.
Primarily mental compulsions
For presentations dominated by mental compulsions, including rumination, mental reviewing, self-reassurance, and neutralising: exposures involve deliberately summoning the feared thought, and response prevention involves not engaging in any mental ritual in response. This is among the most challenging forms of ERP, partly because the compulsions are invisible and partly because stopping a mental behaviour requires noticing it first.
What the Evidence Shows
ERP has been studied more rigorously and over a longer period than almost any other psychological treatment in psychiatry. The evidence is consistent.
ERP: What the evidence shows
~65% of people who complete ERP experience clinically significant symptom reduction
~33% achieve full remission: no longer meeting diagnostic criteria for OCD
12–20 sessions is a standard course; many see meaningful improvement within the first 10
2+ years treatment gains shown to be durable in long-term follow-up studies
Consistently superior to generic CBT, relaxation training, anxiety management, and waitlist controls
When compared to generic CBT without ERP, to relaxation training, to anxiety management, and to waiting lists, ERP is consistently superior. Treatment gains show durability: studies following patients two years after completing ERP show maintenance of gains in the majority of responders.
ERP is not a permanent cure. It is a skill. But it is the skill that changes everything: the ability to face a feared thought without performing a compulsion, and to survive the discomfort that follows.
What Makes ERP Difficult, and Why That Is Worth Knowing
One reason people do not seek ERP, or drop out before completing it, is that no one told them honestly what it involves.
ERP is hard. Not complicated: the principles are simple. But hard in the way that confronting your worst fears repeatedly, without the relief of a compulsion, is hard. In the early stages, anxiety typically increases before it decreases. Your distress level may go up in the first few exposures before your brain begins to learn that it can be managed.
This is not a sign ERP is failing. It is what the process looks like from the inside.
The urge to escape, to check one more time, to seek one more reassurance, to perform one more mental ritual: it will be present and sometimes overwhelming. Research indicates that around a quarter of people who start ERP drop out before completing it, often at this point.
Knowing this in advance matters. Not because it makes the process easier, but because understanding that the discomfort is expected and temporary prevents you from interpreting it as evidence that something is wrong.
ERP is also not something to do alone, particularly in the beginning. Working with a therapist who has genuine expertise in OCD and ERP, not just general CBT training, is important. The hierarchy needs to be built correctly. The exposures need to be specific enough. The response prevention needs to be complete rather than partial. A skilled therapist can also identify subtle avoidance and subtle compulsions that you may not recognise in yourself.
ERP is available in India, but the number of therapists with genuine OCD-specific ERP training remains limited relative to the population. When seeking ERP in India, ask specifically whether the therapist has OCD-specific training and experience. General CBT training is not the same thing.
ERP, Medication, and Other Treatments
ERP and medication for OCD (primarily SSRIs) are not competing treatments. They work through different mechanisms and can be used together.
For mild to moderate OCD, ERP alone is generally recommended as the first-line treatment. For moderate to severe OCD, the evidence supports combining ERP with medication. SSRIs can reduce the intensity of intrusive thoughts and lower baseline anxiety to a level where ERP becomes more manageable. Research shows that ERP alone and ERP combined with medication both outperform medication alone.
Whether to take medication, which medication, and at what dose are decisions for you and your psychiatrist. ERP does not require medication to work. But for some people, particularly those with severe OCD or significant comorbid depression, medication makes the ERP process more accessible.
What about EMDR?
For some people, OCD does not exist in isolation. Where OCD is intertwined with past trauma, ERP alone may be harder to engage with before the underlying traumatic material has been addressed. EMDR (Eye Movement Desensitisation and Reprocessing) is an evidence-based therapy for trauma and PTSD, and there is growing clinical evidence supporting its use as a complementary pathway in trauma-complicated OCD presentations, not as a replacement for ERP, but as preparation for it. The right approach always depends on a proper clinical assessment.
The Bottom Line
If you have OCD and you have not tried ERP, you have not yet tried the treatment most likely to help you.
That is not a judgment. ERP is hard to access in India, it is often badly explained, and its reputation for being frightening puts people off before they start. But the evidence is not marginal or provisional. Decades of randomised controlled trials across multiple countries, OCD presentations, and severity levels consistently find that ERP works, and that it works significantly better than most alternatives.
The goal of ERP is not to eliminate intrusive thoughts. They may continue to arrive. The goal is to change your relationship with them: to reach a point where a feared thought appears, you recognise it as OCD, and you choose not to perform a compulsion. Not because the anxiety has disappeared, but because you have learned, through repeated experience, that you can survive it.
That is a skill. It can be learned. And it changes things.
Frequently Asked Questions
What is ERP therapy?
ERP (Exposure and Response Prevention) is the gold-standard treatment for OCD. It involves deliberately confronting the thoughts, situations, or objects that trigger your OCD (exposure) while choosing not to perform the compulsion that would normally follow (response prevention). Through repeated practice, the brain learns that the feared outcome does not occur and that anxiety can be survived without a compulsion.
Is ERP available in India?
ERP is available in India, but the number of therapists specifically trained in OCD and ERP is significantly limited relative to the population. Most therapists offering OCD treatment have general CBT training, which is not the same. When seeking ERP therapy in India, ask specifically whether the therapist has OCD-specific ERP training and experience. Digital tools like breakOCD are designed to provide ERP-grounded support while you find the right specialist.
Does ERP work for all types of OCD?
Yes. ERP is effective across all OCD presentations including contamination, checking, harm OCD, ROCD, religious OCD, and primarily obsessional OCD among others. The form the exposures take differs depending on the OCD type, but the underlying mechanism is the same. Even for primarily obsessional OCD with mental compulsions, imaginal exposures and response prevention of mental rituals are effective.
How long does ERP take?
A standard course of ERP involves approximately 12 to 20 sessions, typically weekly or fortnightly. Many people begin to see meaningful symptom reduction within the first 10 sessions. The full course typically spans three to five months. Between-session practice is a significant part of treatment, so the time investment extends well beyond the therapy hours themselves.
When do you need medication for OCD?
Medication, primarily SSRIs such as fluoxetine, sertraline, or fluvoxamine, is typically considered when OCD is moderate to severe, when ERP alone has not produced adequate improvement, or when significant comorbid depression is present. For mild OCD, ERP alone is usually the recommended first step. The decision about whether medication is appropriate should be made with a psychiatrist who has experience treating OCD.
Is ERP therapy painful or frightening?
ERP involves encountering anxiety-provoking situations deliberately, which is uncomfortable. In the early stages, distress levels typically increase before they decrease as the brain learns through experience. However, ERP is gradual and hierarchical: you do not start with your worst fears. You start where the anxiety is manageable and build from there. The discomfort of ERP is real. The outcome of not doing it, years of OCD managing your life, is typically far more so.
Can I do ERP without a therapist?
Self-guided ERP is possible and research suggests it can be effective for mild to moderate OCD. However, it is significantly harder without a therapist to help build the hierarchy correctly, identify subtle compulsions, and support you through the most difficult exposures. For moderate to severe OCD, working with an ERP-trained therapist is strongly recommended. Tools like breakOCD's Delay Compulsion Timer and Isha are designed to support ERP principles between therapy sessions, or for those who cannot immediately access a specialist.
Sources & Further Reading
International OCD Foundation: ERP for OCD
PubMed Central: Exposure and Response Prevention for OCD: Current Perspectives
PubMed Central: ERP for OCD: Review and New Directions
Journal of Obsessive-Compulsive and Related Disorders: A systematic review and meta-analysis on the effectiveness of ERP for OCD
Clinical Psychology Review: Inhibitory learning approaches to exposure therapy — a critical review and translation to OCD
PubMed Central: An overview of Indian research in OCD