
Why Does OCD Feel So Real Even When You Know It Makes No Sense?
The brain science behind OCD's convincing grip, and why thinking harder is not the answer
Written by Armaan Raheja, Founder of breakOCD | Clinically reviewed by Dr. Shorouq Motwani, Psychiatrist, Mumbai
In This Article
- The Brain Does Not Treat All Thoughts Equally
- Why Logic Cannot Switch Off the Alarm
- The Role of Inferential Confusion
- Memory Distrust and the Checking Paradox
- Why OCD Targets What Matters Most to You
- The Cycle That Keeps OCD Feeling Real
- What OCD Feels Like in India Specifically
- Why Thinking Harder Never Works
- What Actually Changes the Feeling
- Frequently Asked Questions
You know, logically, that your fear probably is not true. You have told yourself this a hundred times. And it still feels completely real. This is not a weakness. This is OCD working exactly as it is designed to work.
If you live with OCD, you have probably experienced one of its most frustrating contradictions. On one level you know your fear does not make sense. You can see the logic. You can list the reasons why the feared outcome is unlikely. You can tell yourself, accurately, that the thought is just a thought.
And yet none of that knowledge makes the fear go away.
The anxiety does not respond to your reasoning. The doubt keeps returning. The urge to check, seek reassurance, or perform some mental ritual remains just as strong, sometimes stronger, after you have argued against the thought than before.
This experience is a direct consequence of how OCD affects the brain. Understanding why OCD feels so real is not just intellectually interesting. It is clinically important, because it explains why logic alone is never the solution and what actually needs to change.
The Brain Does Not Treat All Thoughts Equally
To understand why OCD feels so real, it helps to understand what is happening in the brain when an intrusive thought arrives.
The human brain has a threat detection system whose primary job is to keep you safe. When it detects something that might be dangerous, it triggers an immediate emotional and physical response. Heart rate increases. Attention narrows. Stress hormones are released. The body prepares to respond.
This system is extraordinarily fast and operates below the level of conscious thought. It does not wait for you to reason through whether the threat is real. It responds first and asks questions later.
In OCD, this threat detection system misfires. Neuroimaging research has identified specific brain circuits consistently implicated in OCD, including the orbitofrontal cortex, which is involved in evaluating potential threats and errors, the anterior cingulate cortex, which signals that something is wrong and demands attention, and the basal ganglia, which regulates habit formation and the completion of behavioral sequences.
In people with OCD, these circuits are hyperactive. The error detection system fires too easily and too loudly. Harmless intrusive thoughts get flagged as significant threats. The brain generates the same alarm response for a random unwanted thought as it would for a genuine danger.
The result is that the feeling of threat arrives before reasoning even begins. By the time your logical mind tries to evaluate whether the fear is real, your body is already in a state of distress. And a distressed brain is much harder to reason with than a calm one.
OCD does not feel real because you are irrational. It feels real because your brain's alarm system is firing at the wrong things. Logic arrives after the alarm. That is too late to prevent the feeling.
Why Logic Cannot Switch Off the Alarm
This is the point that most people with OCD find most frustrating, and it is the most important thing to understand.
OCD does not live in the logical part of the brain. It lives in the emotional learning systems. These systems do not respond to arguments. They respond to experience.
Think of it this way. If you are terrified of dogs because of a bad experience in childhood, someone explaining to you that most dogs are friendly will not make you feel calm when a large dog runs toward you. Your body has already learned that dogs are dangerous. That learning is stored in the emotional memory system. Logic, stored in a completely different part of the brain, cannot simply overwrite it.
OCD works by the same principle. The brain has learned, through repeated cycles of anxiety and compulsion, that certain thoughts are dangerous and require a response. That learning is stored emotionally. Telling yourself the thought is irrational is a logical intervention applied to an emotional problem. It does not reach the part of the brain that is generating the distress.
This is also why people with OCD who try to reason their way through an intrusive thought often find themselves getting more anxious rather than less. The act of engaging with the thought, even to argue against it, signals to the brain that the thought is worth attending to. The alarm gets louder rather than quieter.
Arguing with OCD is like trying to convince a fire alarm that there is no fire. The alarm does not process arguments. It responds to whether the threat system has been reset. That requires a different approach entirely.

The Role of Inferential Confusion
There is a specific cognitive process that researchers have identified as central to why OCD feels so convincing. It is called inferential confusion, and it describes the tendency in OCD to confuse an imagined possibility with a perceived reality.
In everyday thinking, we rely primarily on what we can observe with our senses to judge what is real. If the stove is off, we can see it is off and move on.
In OCD, the imagined possibility overrides sensory evidence. The person knows the stove is off. They checked it. They can see it is off. But the imagined possibility, what if I missed something, what if there is a fault I cannot detect, feels so vivid and urgent that it carries more weight than the direct sensory evidence in front of them.
Inferential confusion is not limited to contamination or checking OCD. It runs through all OCD presentations. A person with harm OCD knows they have never harmed anyone. But the imagined possibility that they might, that something in them might snap, feels more real to them than the evidence of their entire lifetime of behavior. A person with relationship OCD knows their partner has given them no real reason for concern. But the imagined doubt, what if I do not really love them, what if this is not right, overrides everything they can actually observe.
This is why OCD has been described as a disorder of imagination overpowering reality. The brain treats the feared scenario as if it is happening or as if it is genuinely imminent, regardless of what the actual evidence shows.
Memory Distrust and the Checking Paradox
One of the most puzzling experiences people with OCD describe is that the more they check something, the less certain they feel. They check the lock once and feel uncertain. They check it again and feel more uncertain. They check it a third time and the certainty is gone completely.
This is not a failure of memory. It is a well-documented phenomenon in OCD research. Repeated checking reduces the vividness and clarity of memory rather than strengthening it. Each time you return to check, you are implicitly sending your brain a message: my memory of the last check cannot be trusted. Over time the brain stops trusting its own records of what was checked, which creates more doubt, which triggers more checking.
The same process operates with mental compulsions. The more you replay a memory to confirm nothing bad happened, the less clear and reliable the memory feels. The more you check your own feelings to see if they are real, the more uncertain your feelings become. The compulsion that was meant to create certainty actively destroys it.
This is one of the reasons OCD is so difficult to manage through willpower alone. The instinctive response to doubt, checking more thoroughly, produces exactly the opposite of what it intends.
In OCD, checking does not create certainty. It creates more doubt. Every check teaches the brain that the previous check could not be trusted. The only way out of the loop is to stop feeding it.
Why OCD Targets What Matters Most to You
Another reason OCD feels so convincing is that it does not attach to things that are irrelevant to you. It attaches to what you care about most deeply. And things that matter deeply are harder to dismiss.
Research consistently shows that OCD intrusive thoughts center on themes that are personally significant, areas of morality, faith, relationships, responsibility, identity, and safety. These are not random topics. They are the areas of life where the stakes feel highest and where uncertainty feels most unacceptable.
For someone who values being a good parent above everything, the intrusive thought might involve harm to a child. For someone whose faith is the center of their life, the thought may be blasphemous. For someone who has built their identity around being a moral person, the thought will challenge their morality.
This is why OCD thoughts feel so personal, even though they are not chosen. They are designed by the disorder to feel maximally threatening to the specific person experiencing them. The more something matters, the more emotionally charged a thought about it becomes, and the more real the threat feels.
In India, where family honor, religious devotion, and moral character carry particular cultural weight, this dynamic is especially pronounced. OCD finds the thing that matters most and makes it the subject of the doubt. That is not a coincidence. It is the mechanism.
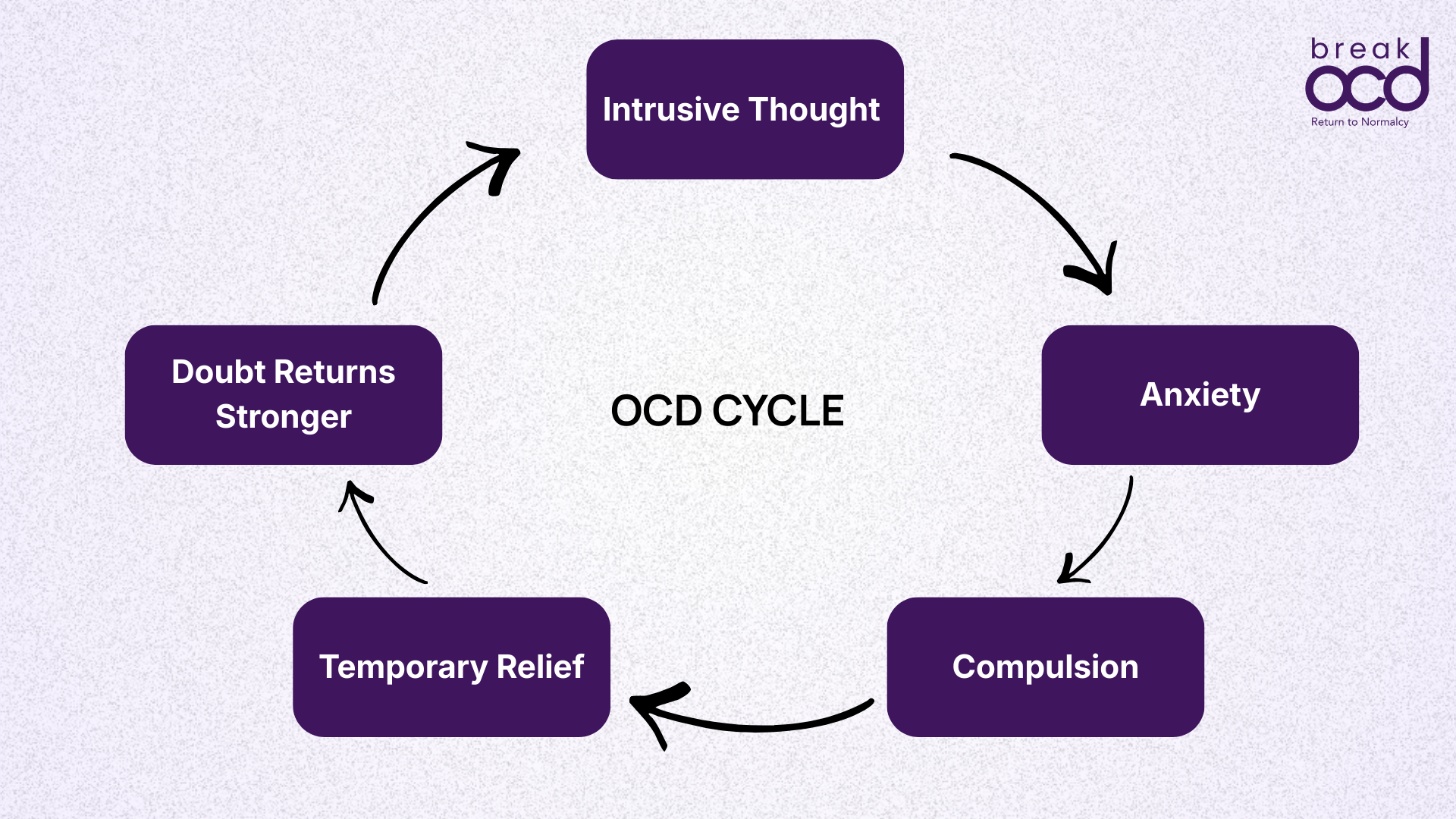
The Cycle That Keeps OCD Feeling Real
Understanding why OCD feels real also requires understanding how the cycle maintains and strengthens that feeling over time.
Every time an intrusive thought arrives and a compulsion is performed in response, two things happen simultaneously. The anxiety drops temporarily, which feels like relief. And the brain records that the compulsion was necessary to produce that relief.
This is operant conditioning. The brain learns: threat appeared, compulsion performed, threat neutralized. Repeat.
Over time this process has several effects that make OCD feel increasingly real:
The threshold for triggering the alarm gets lower. Thoughts that once passed unnoticed now generate significant anxiety.
The range of triggers widens. More situations, objects, and thoughts become associated with the alarm.
The required compulsion escalates. What once took one check now takes five. What once took a brief reassurance now takes an hour of research.
The brain's confidence in its own threat assessment increases. Each compulsion confirms that the threat was real enough to respond to.
This is why OCD tends to worsen without treatment. The cycle is self-reinforcing. The brain is not malfunctioning randomly. It is learning, accurately, from the responses it receives. The problem is that the responses it is receiving are teaching it the wrong lessons.
What OCD Feels Like in India Specifically
India's cultural landscape shapes how OCD presents and how real it feels in specific ways that deserve naming.
Research from NIMHANS, India's premier mental health institution, has documented that religious and moral obsessions are among the most prevalent OCD presentations in Indian populations. Studies of both adult and juvenile OCD in India consistently show high rates of religious obsessions and aggression-related obsessions, themes that carry enormous emotional weight in a culture where devotion and family responsibility are central values.
The result is that for many people with OCD in India, the intrusive thoughts feel not just personally threatening but spiritually and morally catastrophic. A blasphemous thought does not just feel unpleasant. It feels like evidence of spiritual failure. A thought about harming a parent does not just feel disturbing. It feels like a violation of the deepest values a person holds.
This amplification of meaning makes the thoughts feel more real and more urgent than they would in a cultural context where these themes carry less weight. It also makes it harder to seek help, because disclosing the content of the thoughts feels like admitting to something deeply shameful.
Understanding that the emotional intensity of an OCD thought is shaped by what the thought targets, not by any reality behind it, is particularly important in this context. The thought feels catastrophic because it attacks something precious. That is the mechanism of OCD. It is not evidence that the thought is true.
Why Thinking Harder Never Works
People with OCD are often intelligent, thoughtful, and highly analytical. They tend to believe that if they think about the feared thought carefully enough, they will find the certainty they are looking for.
This is one of OCD's most effective traps.
The act of thinking carefully about an intrusive thought, analyzing it, testing it, arguing against it, is itself a mental compulsion. And like all compulsions, it provides temporary relief while reinforcing the cycle. Every minute spent trying to reason away the thought teaches the brain that the thought required that level of attention. The thought becomes more significant, not less.
This is why people who try to logic their way out of OCD often describe feeling like they are running on a treadmill. More effort, same place. The reasoning feels productive but produces no lasting relief. The doubt returns, and the analysis begins again.
The solution is not to think better about the thought. It is to respond differently to the thought. To allow it to exist without engaging it. To let the alarm ring without treating it as an emergency. This is exactly what ERP teaches the brain to do.
What Actually Changes the Feeling
If logic does not change how real OCD feels, what does?
The answer is new emotional experience, not new information. The brain changes what it believes is dangerous not when it is told something is safe but when it repeatedly experiences safety in the presence of the feared stimulus without the compulsion occurring.
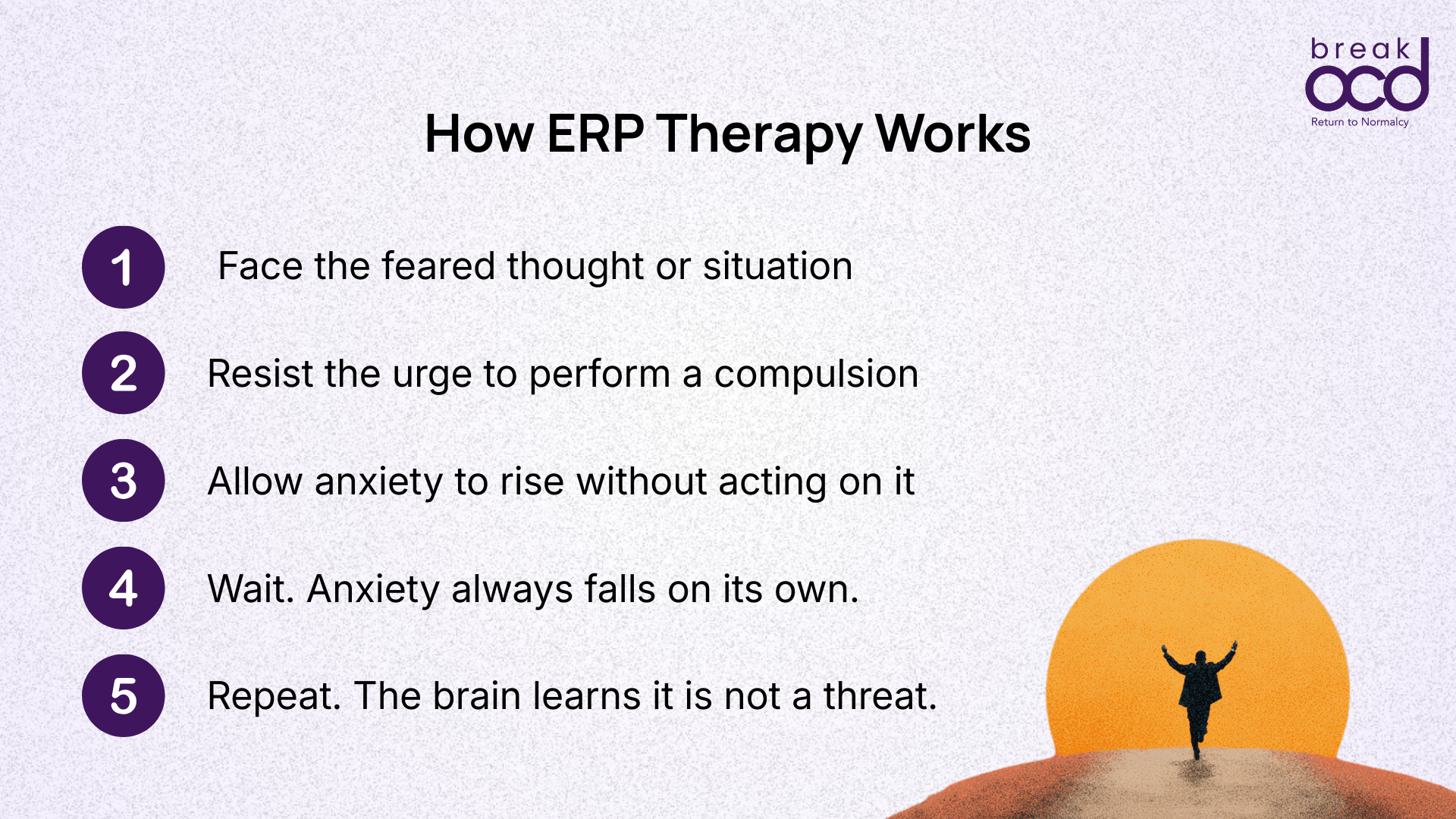
This is the foundation of Exposure and Response Prevention therapy, ERP. In ERP, a person deliberately faces the intrusive thought or the feared situation without performing the compulsion. The anxiety rises. And then, without the compulsion intervening, it naturally falls on its own. The brain has a new experience: the thought arrived, no compulsion was performed, and nothing catastrophic happened. The alarm system begins to recalibrate.
This process does not happen after one exposure. It requires repetition, because the emotional learning system needs multiple experiences to update its threat map. But over time the change is real and often profound. The same thought that once generated overwhelming anxiety becomes, eventually, just a thought.
Recovery from OCD does not mean the thoughts stop arriving. Intrusive thoughts are a normal part of being human. Recovery means the thoughts stop feeling like emergencies. They stop commanding a response. And in that shift, a great deal of life that OCD had occupied becomes available again.
Frequently Asked Questions
Why does OCD feel real even when I know it is irrational?
Because OCD operates in the emotional learning systems of the brain, not the logical ones. The brain's threat detection circuit fires before conscious reasoning begins, generating a felt sense of danger that logic arrives too late to prevent. Knowing something is irrational and feeling safe are processed by different parts of the brain. OCD exploits the gap between them.
Why does arguing with my OCD thoughts make the anxiety worse?
Engaging with an intrusive thought, even to argue against it, signals to the brain that the thought is significant enough to require attention. This reinforces the neural pathway that connects the thought to the alarm response. Every analysis, however logical, is also a compulsion that teaches the brain to treat the thought as a threat. The more you argue, the louder the alarm becomes.
Why does checking make me feel less certain rather than more?
This is a well-documented phenomenon in OCD research. Repeated checking reduces the clarity and vividness of memory rather than strengthening it. Each time you return to check, you implicitly tell your brain that the previous check was not trustworthy. Over time the brain stops trusting its own records, which generates more doubt and more checking. The compulsion produces the opposite of its intended effect.
Does the fact that OCD feels so real mean my fears might actually be true?
No. The intensity of the feeling is generated by the brain's misfiring threat system, not by the accuracy of the feared scenario. OCD consistently targets what matters most to a person, which is exactly why the thoughts feel so personally significant and urgent. The emotional charge is a product of the mechanism, not evidence of the content. A thought can feel completely real and still be completely wrong.
If logic does not help, what does?
New emotional experience is what changes how real OCD feels. The brain updates its threat assessment not when it receives new information but when it repeatedly experiences safety in the presence of a feared thought without a compulsive response. This is what ERP therapy provides: structured, repeated experiences that teach the brain the thought is not an emergency and does not require action.
About the Author
Armaan Raheja
Armaan Raheja is the founder of breakOCD, India's first dedicated OCD support app. He was diagnosed with OCD after years of misdiagnosis and went on to study psychology in the United States, where he received evidence-based treatment including ERP therapy. On returning to India and finding a fragmented mental health system with few OCD-specific resources, he built breakOCD to provide the support he wished had existed. Armaan brings both lived experience of OCD and a commitment to evidence-based, stigma-free mental health care in India.
Clinically Reviewed By
Dr. Shorouq Motwani
Dr. Shorouq Motwani is a Psychiatrist in Mumbai. She specializes in emotional and behavioral disorders, neurodevelopmental disorders, and mental health in adolescents and young adults. She is the recipient of the ASHA Award for best paper presentation and has multiple published research papers in psychiatry.
Sources & Further Reading
International OCD Foundation: What is OCD
NHS: Obsessive Compulsive Disorder Overview
Government of India: Rights of Persons with Disabilities Act 2016
NIMHANS: An Overview of Indian Research in Obsessive Compulsive Disorder