
Mental Compulsions in OCD: The Invisible Rituals Keeping You Stuck
Why the most common form of OCD is also the least recognized
Written by Armaan Raheja, Founder of breakOCD | Clinically reviewed by Jehanzeb Baldiwala, Psychologist, Mumbai
In This Article
- What Mental Compulsions Actually Are
- Common Types of Mental Compulsions
- Why Mental Compulsions Feel Like Thinking
- Why Mental Compulsions Are Especially Common in India
- The OCD Cycle with Mental Compulsions
- Why Mental Compulsions Are Missed and Misdiagnosed
- What Treatment Looks Like for Mental Compulsions
- Frequently Asked Questions
You have probably spent hours trying to figure out if what you are thinking means something. Going over the same memory again and again. Telling yourself you are a good person until it feels true. That is not just thinking. That is OCD.
When most people picture OCD, they picture visible behavior. Hand washing. Checking locks. Arranging objects. These images are so embedded in the popular understanding of OCD that many people with the condition spend years not recognizing themselves in them.
What they do not picture is someone sitting quietly, looking completely fine, while running an exhausting loop of mental rituals that has been going for hours. Replaying a conversation. Mentally reviewing their own intentions. Counting silently. Replacing a bad thought with a good one. Praying until it feels right. Checking their own feelings to see if they are real.
These are mental compulsions. They are invisible, extremely common, and one of the most significant reasons OCD goes unrecognized in India and globally.
A cross-sectional study conducted across OCD patients in Karnataka found that mental compulsions were present in more than half of all participants, with the most common forms being mentally undoing bad thoughts with good ones, praying, and self-reassurance. Despite this prevalence, mental compulsions remain underdiagnosed and undertreated, partly because the standard clinical tools for measuring OCD were not originally designed to capture them.
Understanding mental compulsions is often the turning point at which everything finally makes sense.
What Mental Compulsions Actually Are
A compulsion in OCD is any behavior, mental or physical, performed in response to an intrusive thought with the intention of reducing anxiety, gaining certainty, or preventing something bad from happening.
Mental compulsions are compulsions that happen entirely inside the mind. There is no observable behavior. From the outside, the person looks still. Internally, they are engaged in a repetitive mental ritual that follows the same function as any visible compulsion.
What makes mental compulsions so difficult to recognize is that they look and feel like thinking. Normal, reasonable, responsible thinking. The person is not aware they are performing a compulsion. They believe they are problem-solving, being careful, or simply trying to understand themselves better.
This is the defining trap of mental compulsions. They do not feel irrational. They feel necessary.
Mental compulsions do not feel like rituals. They feel like thinking. That is exactly what makes them so hard to catch and so hard to stop.

Common Types of Mental Compulsions
Mental compulsions vary widely in form but share the same underlying function. All of them are attempts to reduce the anxiety or uncertainty produced by an intrusive thought.
Rumination
Endlessly analyzing a thought, feeling, memory, or situation in an attempt to reach a conclusion, gain certainty, or understand what the thought means. Rumination feels like deep thinking but never arrives at resolution. The same question loops without a satisfying answer, because in OCD there is no answer that feels certain enough to stick.
Mental Reviewing
Replaying a past event, conversation, or interaction in the mind to check whether something wrong occurred. Someone with harm OCD may replay an entire day to confirm they did not hurt anyone. Someone with relationship OCD may replay a conversation to confirm they said the right things and felt the right feelings.
Mental Checking
Repeatedly scanning one's own emotions, sensations, or intentions to verify they are correct. This might involve checking whether you still love your partner, checking whether a bodily sensation is a sign of illness, or checking whether an intrusive thought was accompanied by arousal or desire. The checking provides momentary information but never permanent certainty, so it is repeated.
Thought Neutralization
Attempting to cancel or undo a bad thought by deliberately replacing it with a good one. For example, having an intrusive thought about harming someone and immediately countering it with an image of kindness or love. The Indian clinical study mentioned above found this to be the most common mental compulsion in their sample, present in over half of participants with mental compulsions.
Praying as Compulsion
Repeating a prayer or religious phrase until it feels perfectly right or sufficient. This is distinct from sincere prayer, which is an expression of faith. Compulsive praying in OCD is driven by anxiety and feels incomplete until performed with a specific quality of feeling or exactness. It must be done again if the feeling is not quite right. In India, where religious practice is central to daily life across many communities, this form of mental compulsion is particularly prevalent and particularly easy to miss.
Mental Reassurance
Silently telling yourself that you are a good person, that nothing bad will happen, or that the feared outcome is not real. This is the internal version of reassurance seeking, and it functions identically. The relief it provides is temporary. The doubt returns, and the reassurance must be repeated.
Counting and Repeating
Mentally counting to a specific number, repeating a phrase a set number of times, or going through a sequence of thoughts until a feeling of completeness or rightness is achieved. These compulsions often have a felt quality attached to them. The ritual is not finished until it feels finished, and if something interrupts it, it must begin again.
Why Mental Compulsions Feel Like Thinking
The reason mental compulsions are so difficult to identify is that the mind uses the same cognitive machinery for genuine reflection and for compulsive rumination. Both involve sustained attention to a thought. Both feel purposeful. Both can look identical from the outside.
The distinction lies in what the process produces.
Genuine reflection leads somewhere. You think about a problem, reach a conclusion or acceptance, and move on. The thought does not demand you return to it.
Mental compulsions loop. The thought returns. The question resurfaces. No answer feels sufficient. The process generates more anxiety over time, not less, because the act of repeatedly engaging with a thought signals to the brain that the thought is important and dangerous.
A useful question to ask yourself: is this thinking moving me forward, or is it keeping me in the same place? Reflection produces movement. Rumination produces more rumination.
This distinction matters enormously in OCD because many people with mental compulsions have been told they are overthinkers, or that they need to stop dwelling, or that they are too sensitive. These descriptions are not accurate or helpful. Mental compulsions are not a character trait or a cognitive style. They are a learned response to anxiety that can be unlearned with the right treatment.
Why Mental Compulsions Are Especially Common in India
The Karnataka study cited above found that among patients with mental compulsions, the most prevalent obsession themes were religious or sacrilegious thoughts, followed by symmetry and harm-related obsessions. The most common mental compulsions were thought neutralization, praying, and self-reassurance.
These findings reflect something that clinicians working in India have observed for years. Mental compulsions are not simply a Western clinical phenomenon. They are deeply embedded in how OCD presents in Indian populations, shaped by the cultural and religious context in which they develop.
In a country where faith is central to daily life, where prayer is woven into morning routines, and where religious obligation is a source of both comfort and responsibility, compulsive praying can go unnoticed for years. It looks like devotion. The person performing it often experiences profound shame precisely because they sense it is not sincere prayer but cannot stop.
Similarly, the high premium placed on being a good person in Indian family and community culture means that mental checking of one's own intentions and moral standing is extremely common. Someone who genuinely cares about being a good son, daughter, spouse, or community member is more likely to have OCD target that very concern.
The result is that mental compulsions in India are often invisible not just to the person experiencing them, but to the families around them, and sometimes to clinicians who are not specifically trained in OCD.
The OCD Cycle with Mental Compulsions
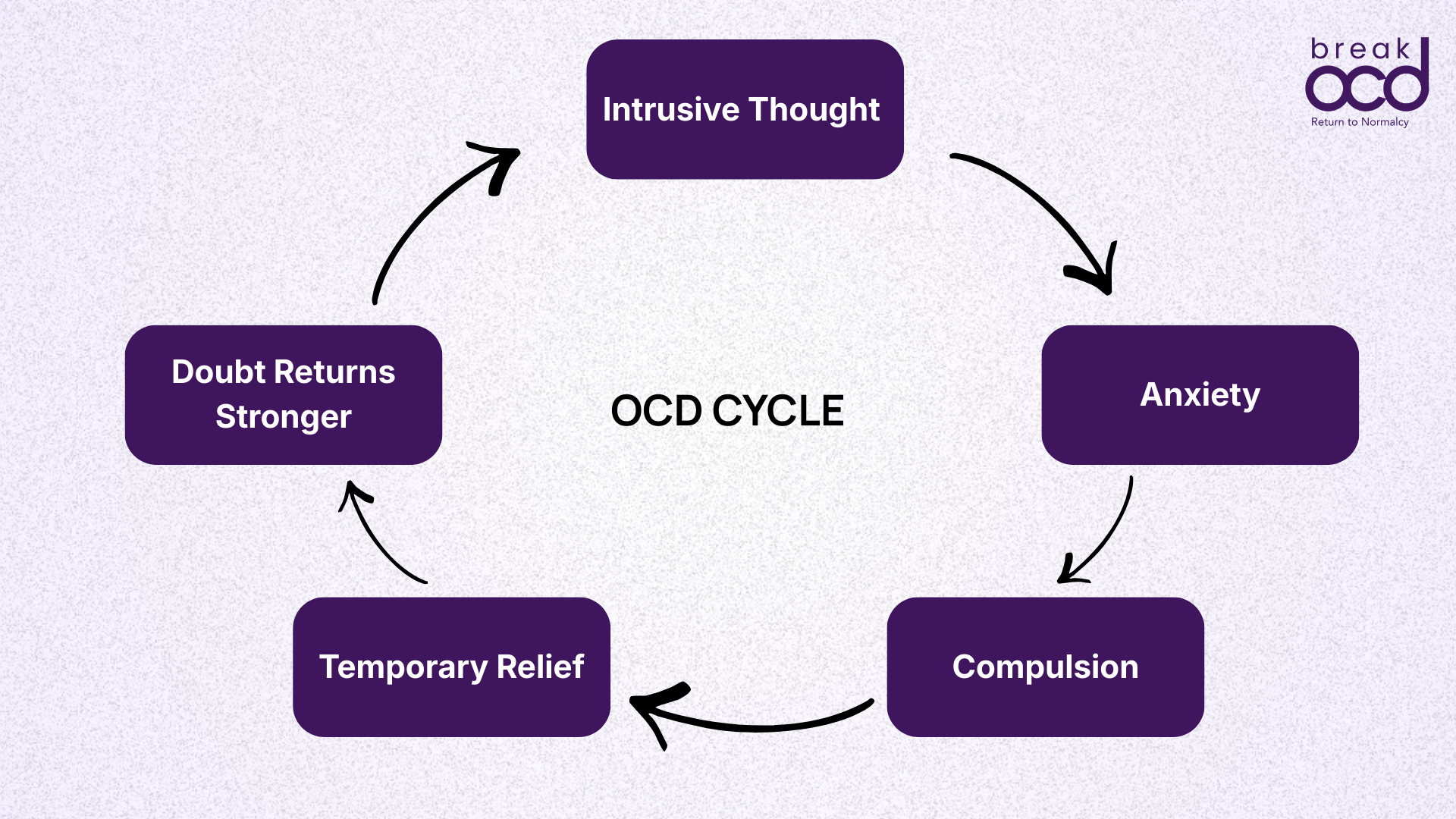
Mental compulsions follow the same cycle as all OCD compulsions. Understanding this cycle is what allows a person to begin to step outside it.
An intrusive thought arrives, perhaps a doubt about a past action, a fear about a relationship, or a disturbing image
Anxiety and discomfort spike immediately
The mind begins a mental ritual: reviewing, analyzing, neutralizing, reassuring, counting, or praying
Anxiety drops temporarily
The brain records that the mental ritual produced safety
The thought returns, often stronger, because engaging with it confirmed its importance
The urge to perform the mental ritual increases
What makes this cycle particularly stubborn is that mental compulsions are available at all times. There is no lock to check, no sink to use, no action to take. The ritual is always accessible. It can run in the background of any activity, in any location, without anyone else knowing. This means there are fewer natural interruptions to the cycle than there might be with a physical compulsion.
It also means the compulsions can escalate very quickly. What begins as briefly checking a memory can become hours of mental review before the person fully understands what is happening.
Why Mental Compulsions Are Missed and Misdiagnosed
Because mental compulsions have no visible component, they are frequently missed in clinical settings where assessments focus on observable behavior. The standard clinical tool for measuring OCD, the Yale-Brown Obsessive Compulsive Scale, was historically weak at capturing mental rituals, which the Karnataka study identified as one of the reasons mental compulsions are likely underestimated in research populations.
In India specifically, several additional factors contribute to misdiagnosis:
The person presents with anxiety or depression symptoms, which are visible, while the OCD driving them remains undetected
Mental reviewing and rumination are described to clinicians as overthinking or inability to concentrate, which may be attributed to stress or anxiety
Compulsive praying is not recognized as a symptom in religious households where frequent prayer is normal
The shame attached to the content of intrusive thoughts prevents people from disclosing the full picture to a clinician
The result is that many people with predominantly mental compulsions receive treatment for anxiety or depression that does not address OCD, and they do not improve in the ways expected. The frustration of this experience is itself a significant burden.
If you have been told you have anxiety or depression but treatment has not helped the way it should, it may be worth asking specifically about OCD. Mental compulsions are one of the most common reasons the real condition is missed.
What Treatment Looks Like for Mental Compulsions
Exposure and Response Prevention therapy, ERP, is the gold-standard treatment for OCD including mental compulsions. The same principles apply whether the compulsion is physical or mental, but working with mental compulsions requires additional clarity about what the compulsion actually is.
The first step in ERP for mental compulsions is recognition. The person must learn to identify when a mental ritual is starting, which is difficult because the line between thinking and compulsing is not always obvious. This is one of the reasons working with a clinician who specializes in OCD is particularly valuable for mental compulsions.
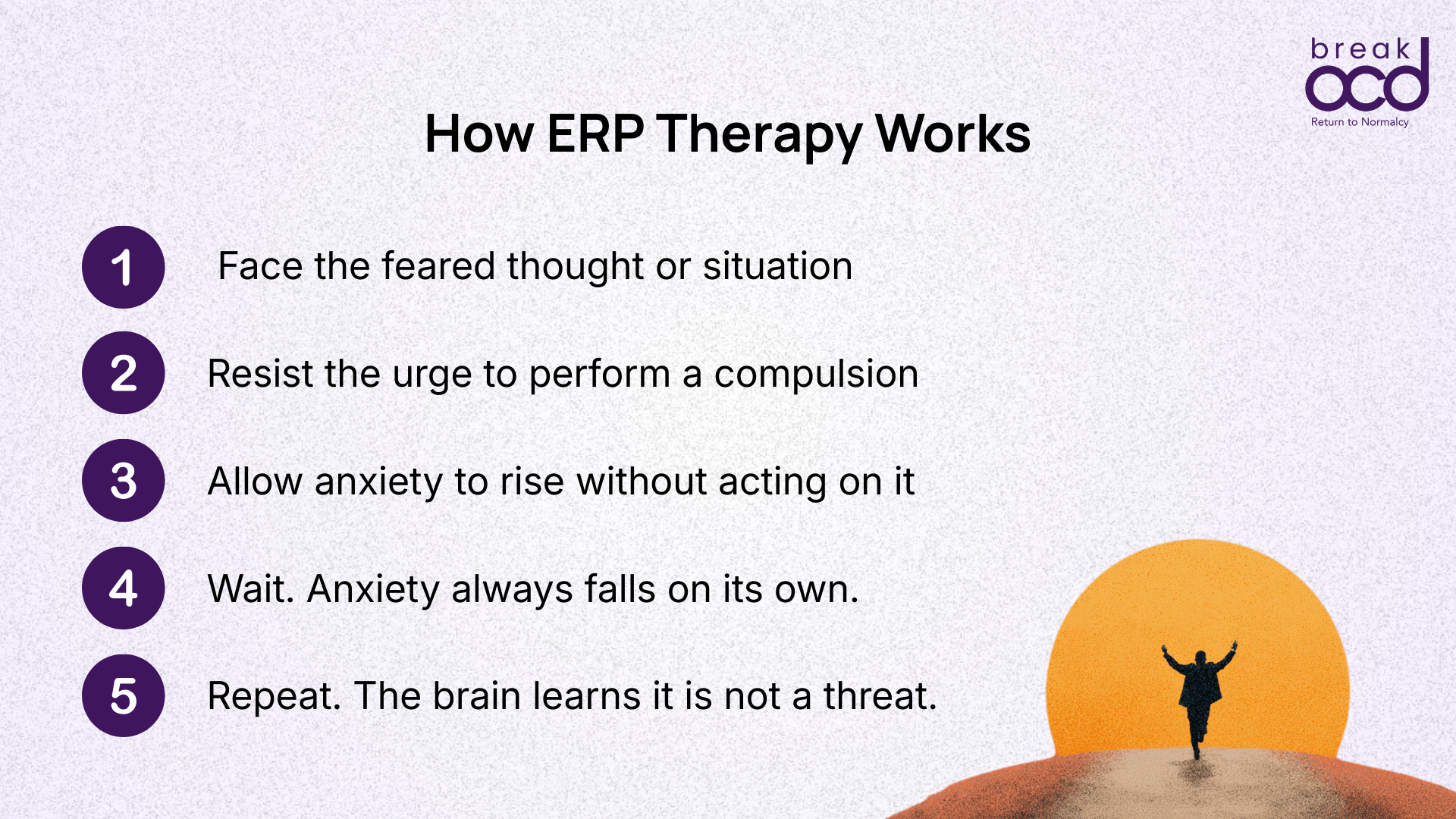
Once identified, the work of ERP involves:
Allowing the intrusive thought to exist without engaging in the mental ritual
Tolerating the anxiety and uncertainty that arises when the compulsion is not performed
Experiencing that anxiety rises and then naturally falls, without the ritual having resolved anything
Gradually reducing the power the thought has by repeatedly demonstrating that it does not require a response
This process is uncomfortable. The brain has learned to expect the ritual and will generate significant anxiety when it does not arrive. The discomfort is not a sign that something has gone wrong. It is a sign that the brain is encountering the uncertainty it has been trained to avoid, and beginning the process of learning that it can survive that uncertainty without acting.
Over time the urge weakens. The thoughts lose their charge. The mental space that was previously occupied by rituals becomes available for the rest of life.
Recovery does not mean thoughts stop arriving. It means they stop demanding a response.
Frequently Asked Questions
What is the difference between rumination and normal reflection?
Normal reflection leads to a conclusion or acceptance and allows the person to move on. Rumination in OCD loops without resolution. The same question returns repeatedly, no answer feels certain enough, and the process generates more anxiety over time rather than less. If you find yourself returning to the same thought or question despite having already thought it through, that is a sign of rumination rather than reflection.
Is Pure O a real diagnosis?
Pure O is not an official clinical diagnosis. It is a colloquial term used to describe OCD in which compulsions are primarily mental rather than physical. Clinically, it is simply OCD. The distinction is useful because it helps people who do not recognize themselves in descriptions of visible rituals understand that OCD can present without any outward behavior. Almost everyone described as having Pure O still has compulsions. They are just invisible.
How do I know if my praying is a compulsion or sincere faith?
The distinction lies in what drives the prayer and what happens if it is not performed or not performed correctly. Sincere prayer is an expression of faith that can be completed and set aside. Compulsive praying in OCD is driven by anxiety, must be repeated until it feels exactly right, and leaves the person feeling worse or more doubtful if it is incomplete. The person performing it often recognizes that something is wrong, even if they cannot name it.
Can mental compulsions be treated the same way as physical compulsions?
Yes. The same principles of Exposure and Response Prevention therapy apply to mental compulsions. The process requires additional work in identifying what the mental compulsion actually is, since the line between thinking and compulsing can be subtle. A clinician trained specifically in OCD will be able to help identify mental compulsions and design exposures that address them directly.
Why have I never heard of mental compulsions before?
Mental compulsions are significantly underrepresented in popular descriptions of OCD, which tend to focus on visible and dramatic symptoms. They are also harder to measure clinically, which means they have historically been underrepresented in research as well. In India specifically, very little publicly available OCD education addresses mental compulsions directly. This is one of the core reasons breakOCD was built: to provide accurate, complete information about how OCD actually presents in Indian people.
Sources & Further Reading
International OCD Foundation: About OCD
NHS: Obsessive Compulsive Disorder Overview
Government of India: Rights of Persons with Disabilities Act 2016
PMC: Assessment of the Prevalence and Types of Mental Compulsions in OCD in North Karnataka