
Religious OCD: When Your Faith Becomes a Source of Torment
Written by Armaan Raheja, Founder of breakOCD | Clinically reviewed by Dr. Sachi Pandya, Psychologist, Mumbai
In this article
You are in the middle of your prayers. And a thought arrives: awful, unbidden, the last thing you would ever want to think in this moment. You try to push it away, but the harder you push, the louder it gets. So you start again. Repeat the prayer. Try to do it right this time. But the thought comes back.
If this sounds familiar, you are not alone. And you are not spiritually corrupted.
What you are describing has a clinical name: scrupulosity. It is a subtype of Obsessive-Compulsive Disorder in which OCD targets a person's religious faith, moral code, or spiritual practice. It is one of the most common presentations of OCD globally, affecting between one quarter and one third of all people with OCD. In highly religious societies, clinical research suggests that figure is even higher. Some studies estimate that religious and moral obsessions affect 50 to 60 percent of people with OCD in those settings.
In India, where faith is woven deeply into the fabric of daily life across communities, religious OCD is particularly prevalent. It is also particularly invisible, because its symptoms are so easily mistaken for the things they are not: excessive devotion, religious sensitivity, or a spiritual problem requiring a spiritual solution.
This article explains what religious OCD actually is, how it presents across different Indian faith traditions, why the most well-intentioned responses make it worse, and what the right treatment looks like.
What Is Religious OCD?
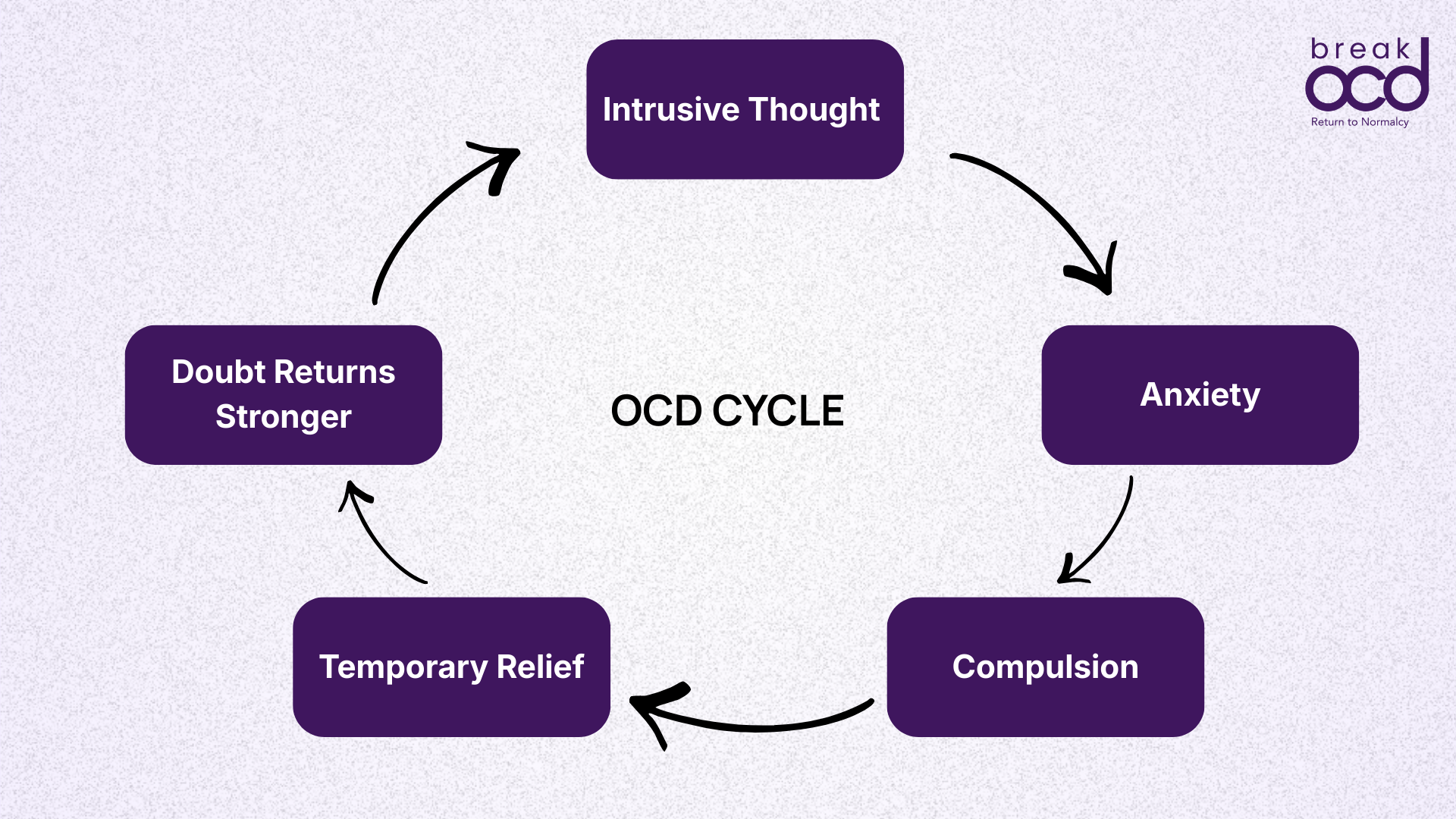
Religious OCD (clinically called scrupulosity) is not about being too religious. It is OCD, the same condition described by the cycle of intrusive thoughts, anxiety, compulsions, and temporary relief, targeting the domain of a person's faith.
The word scrupulosity comes from the Latin scrupulus, meaning a small sharp stone: the sensation of something small but persistently painful. Historically, it was used in Catholic moral theology to describe pathological doubt about sin. Clinically, it now refers to OCD symptoms across any religion or moral framework, including in people with no religious affiliation at all.
The obsessions in religious OCD typically involve:
Unwanted blasphemous thoughts or images that arise during prayer, worship, or sacred moments.
Fear of having committed a sin, often without any evidence of wrongdoing.
Persistent doubt about whether a prayer was performed correctly, sincerely, or in a state of sufficient purity.
Fear of offending God, a deity, or a higher power.
Intrusive sexual or violent images in religious contexts.
Moral obsessions: a persistent sense of having been dishonest, unkind, or ethically wrong, without clear cause.
The compulsions are the behaviours performed in response to this anxiety. They include:
Repeating prayers until they feel right or pure.
Excessive confession: to God, a priest, a parent, a religious leader, or repeatedly in one's own mind.
Seeking reassurance that one has not sinned or that God is not displeased.
Researching religious texts or doctrine to resolve doubt.
Avoiding religious spaces, objects, or rituals out of fear of contaminating them.
Mental reviewing: going over prayers, thoughts, or actions repeatedly to check for errors.
From the International OCD Foundation
OCD never helps with religious practice. It creates barriers to it. A person with religious OCD often appears, to an outside observer, to be deeply devout. But the behaviour is not driven by faith. It is driven by fear.

Why Religious OCD Is Particularly Common in India
India is one of the most religiously diverse and deeply devout countries in the world. For hundreds of millions of people, faith is not a private matter. It is embedded in daily routine, family structure, seasonal calendar, and personal identity. This is not a problem. But it does create specific conditions in which religious OCD can flourish, stay hidden, and cause enormous suffering.
The core reason is clinical: OCD attaches most powerfully to the things that matter most to a person. When faith is central to someone's identity and their sense of being a good person, intrusive thoughts that appear to violate that faith generate extreme distress. And extreme distress fuels the compulsion cycle.
A 2025 study published in Mental Health, Religion and Culture, conducted among OCD patients in Kashmir, found significant associations between OCD severity, scrupulosity, guilt, and religiosity. This confirms what clinicians in India have long observed. The more a person's faith matters to them, the more distressing an intrusive thought becomes, and the harder the OCD works to generate and sustain it.
Hindu communities
In Hindu practice, religious OCD often shows up around puja/pooja. The person may feel compelled to repeat a puja from the beginning if a thought occurred during it, if their concentration slipped, or if a ritual object was touched in the wrong order. Mantras may need to be repeated a precise number of times before they feel complete. The fear of ritual impurity, and the endless checking, washing, or re-doing that follows, can consume hours of a day.
Intrusive blasphemous images during puja are extremely common and extremely distressing. The person does not want these thoughts. They horrify them. But the more they try to suppress them, the more forcefully they return.
Muslim communities
In Islamic practice, a specific concept already exists within Islamic scholarship to describe this experience: waswas, meaning intrusive whispers during salah or other acts of worship. Classical Islamic scholars have traditionally advised ignoring these thoughts and continuing with prayer without responding to them. This guidance is, remarkably, consistent with the ERP approach to religious OCD: tolerate the thought without responding compulsively.
But for many people, the waswas becomes a clinical OCD presentation. Wudu (ritual ablution) must be repeated because it may not have been performed correctly. Salah is repeated because a thought occurred that rendered it invalid. The niyyah (intention) must be reasserted perfectly before any act of worship. The cycle can make the performance of a simple prayer take hours and leave the person exhausted, ashamed, and further from the peace that prayer is meant to provide.
Sikh, Christian, and Jain communities
In Sikh practice, intrusive thoughts during paath (scripture reading or recitation) cause similar distress. In Indian Christian communities, particularly Catholic, confessional compulsions are common: the same sin confessed repeatedly across multiple confessions because the person does not feel sufficiently forgiven, or fears they did not confess correctly. In Jain communities, where non-violence (ahimsa) is the central ethical principle, harm obsessions can become entangled with deep religious guilt: the fear of having accidentally killed a small creature, or of having violent thoughts.
The content differs across traditions. The OCD mechanism is identical.
Why Devout People Suffer More: Thought-Action Fusion
There is a clinical concept that explains why religious OCD tends to be more distressing in people of strong faith. It is called thought-action fusion, and understanding it is one of the most important things a person with religious OCD can do.
Thought-action fusion is a cognitive distortion with two components. The first is the belief that having a thought about something bad makes it more likely to happen, as if the thought itself has causal power. The second, and more relevant here, is the belief that having a thought about something morally wrong is the moral equivalent of actually doing it.
In the context of faith, this means: if I have a blasphemous thought during prayer, I am as guilty as if I committed blasphemy. If I have a violent image about a deity I love, I am as sinful as if I intended harm.
This is clinically false. But in certain religious contexts, there are teachings that appear to support it: that thoughts and intentions carry moral weight. For a deeply religious person with OCD, this creates a catastrophic interaction. The intrusive thought arrives. The OCD generates the belief that the thought is morally equivalent to an act. The person is flooded with guilt, fear, and shame. They perform a compulsion to reduce the guilt. The compulsion provides temporary relief. The thought returns, and now the brain has learned that this thought requires a response.
Research published in PubMed confirms: thought-action fusion is implicated in the development and maintenance of OCD, and certain religious teachings that emphasise moral purity and the significance of thoughts can amplify these beliefs, fuelling the OCD cycle. The religion itself is not the cause. The interaction between thought-action fusion beliefs and the OCD mechanism is.
What is thought-action fusion?
The belief that having a thought about something bad is the moral equivalent of actually doing it.
For someone with religious OCD, this means: if I have a blasphemous thought during prayer, I am as guilty as if I committed blasphemy. This belief is part of the OCD mechanism, not a spiritual truth.
This also explains something that confuses many people with religious OCD: why the intrusive thoughts are most likely to appear precisely in sacred moments. During prayer. In temple. At the moment of communion. During a holy day. This is OCD at work, not a sign of spiritual failure. OCD exploits what matters most. The more sacred the moment, the more violating the intrusive thought feels, and the more powerful the distress. Which is exactly what OCD needs to sustain the cycle.
It Is Not a Spiritual Problem. It Is an OCD Problem.
The most important clinical fact about religious OCD is that its thoughts are ego-dystonic. Ego-dystonic means the thought is completely alien to the self. It conflicts with the person's values, their love for their faith, and their sense of who they are.
The person having blasphemous intrusive thoughts is almost always someone for whom faith matters deeply. The thought horrifies them precisely because it does. The distress is not evidence of spiritual corruption. It is evidence of devotion.
A person who genuinely harbours contempt for their faith does not experience blasphemous thoughts as distressing. The distress is the diagnostic signal. It is what separates an OCD intrusion from an actual belief.
A person with religious OCD is not secretly disrespectful of their faith. They are suffering within it. OCD has found the most protected, most sacred part of their interior life and made it the target of attack.
Having a blasphemous thought during prayer does not mean you are blasphemous. Having an intrusive image of something sacred does not mean you have lost your faith.
The thought is not a reflection of who you are or what you believe. It is a symptom of OCD.
Why the Most Loving Responses Make It Worse
When a person with religious OCD confides in a family member, a religious elder, or a community leader, the response is almost always given with genuine care. And it almost always makes the OCD worse.
Why loving responses make it worse
The typical advice is: pray more. Increase your devotion. Recite this protective verse. Perform this ritual. Seek forgiveness more sincerely. This is loving guidance. And it is functionally a prescription for more compulsions.
Every prayer repeated in response to an intrusive thought confirms to the brain that the thought was real, dangerous, and required a response. This is not a failure of faith on the part of the family. It is a failure of information.
Every prayer repeated in response to the intrusive thought confirms to the brain that the thought was real, dangerous, and required a response. Every confession sought teaches the brain that the thought needed to be resolved. Every ritual performed to restore purity gives the OCD exactly what it needs to continue.
Reassurance from family ("of course you haven't sinned," "God knows your heart," "you're a good person") provides temporary relief and then requires repetition. This is reassurance-seeking, and it is one of the most common compulsions in religious OCD. Each reassurance temporarily quiets the anxiety. Then the doubt returns, slightly stronger than before, requiring a slightly more convincing reassurance. Over time, the person may need many reassurances per day, from multiple people, across multiple conversations.
This is not a failure of faith on the part of the family. It is a failure of information. When families understand that the more helpful response is to gently reduce accommodation rather than reassure and facilitate, outcomes for the person with OCD improve significantly.
What Actually Helps: ERP and the Relationship Between Faith and Treatment
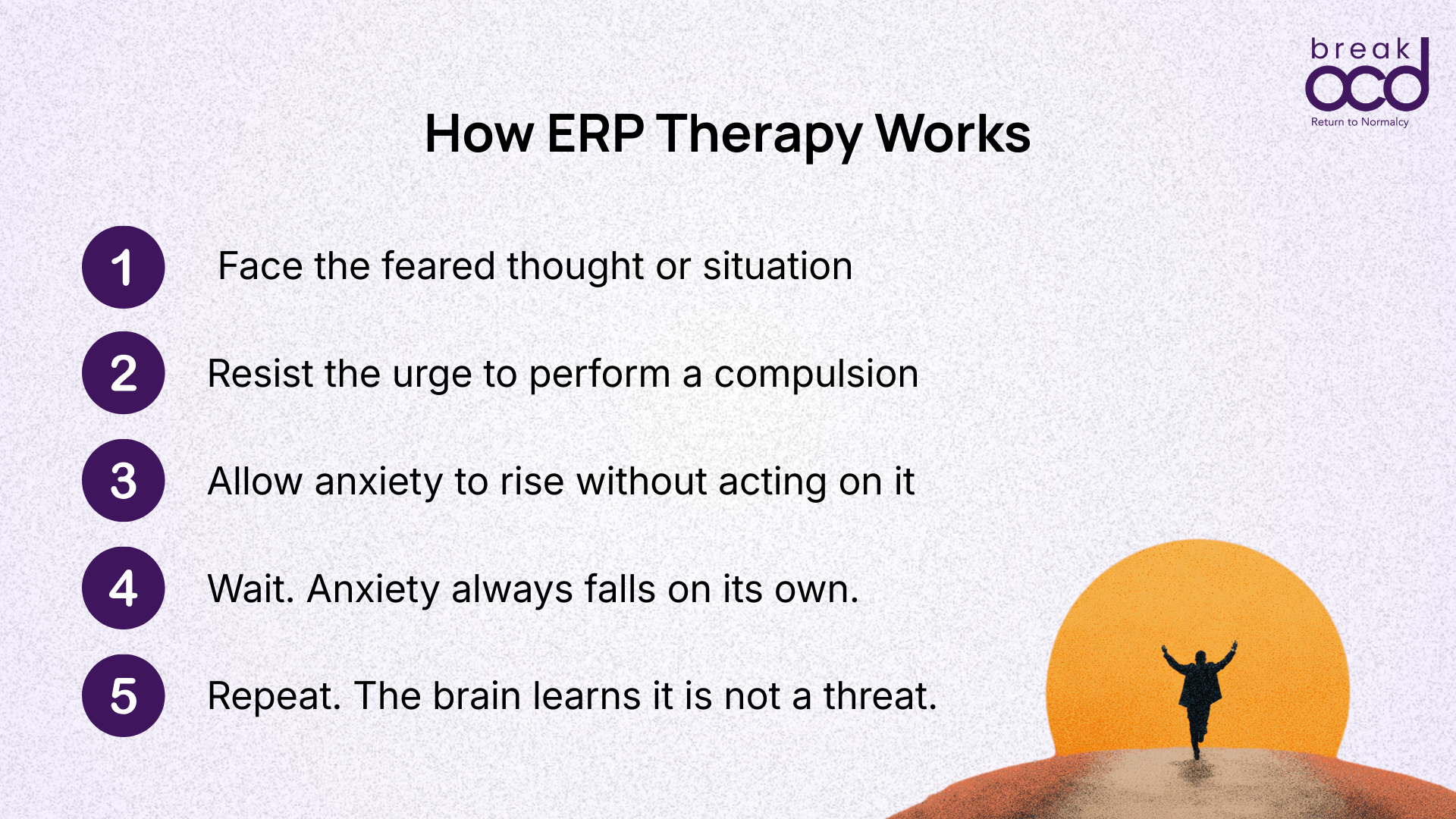
Religious OCD responds to the same treatment as all other forms of OCD: Exposure and Response Prevention (ERP) therapy, often in combination with medication. ERP has the strongest evidence base of any psychological treatment for OCD, and this holds for scrupulosity specifically.
A 2025 systematic review in Current Psychology examining 13 studies on the treatment of scrupulosity found that all psychotherapy-based interventions (including ERP, CBT, and ACT) showed meaningful improvement in religious OCD symptoms. The evidence for ERP is the most robust.
In ERP for religious OCD, the exposures are designed in collaboration with the person and their therapist. They might involve tolerating an intrusive thought during prayer without repeating the prayer. Entering a religious space without performing a ritual beforehand. Allowing a confession to remain unconfirmed without seeking reassurance. The goal is not to make the person think bad thoughts about their faith. It is to allow them to have intrusive thoughts without treating them as meaningful, and to discover through repeated experience that the anxiety reduces without any compulsion being necessary.
Faith and ERP are not in conflict
This is the concern raised most often by people with religious OCD and their families: will treatment require me to disrespect my faith? The answer is no. ERP does not ask anyone to abandon or disrespect their religion. It asks them to stop treating intrusive thoughts as spiritually meaningful. These are different things.
A trained OCD therapist, particularly one familiar with the cultural and religious context, can conduct ERP in a way that is respectful of a person's faith. There are clinicians who incorporate the person's religious understanding into the therapeutic framework, helping them see that the OCD is what is attacking their faith, not the treatment.
Many people with religious OCD report that following successful ERP treatment, they are able to practise their faith with more peace, presence, and genuine connection than they experienced before. The OCD was not protecting their faith. It was consuming it.
You do not have to choose
You do not need to choose between your faith and your recovery. ERP is not an attack on what you believe. It is a clinical tool designed to separate the OCD from your religion, so that you can be present in your practice rather than trapped in a cycle.
Many people with religious OCD report that following successful ERP treatment, they are able to practise their faith with more peace, presence, and genuine connection than they experienced before. The OCD was not protecting their faith. It was consuming it.
When Should You Seek Help?
Religious OCD often goes unrecognised for years, sometimes decades, because it looks like devotion, and because the shame associated with intrusive thoughts in sacred contexts makes disclosure difficult. People with religious OCD frequently do not tell their doctor what they are experiencing because they fear the thoughts will be judged rather than recognised as symptoms.
It is worth seeking a clinical assessment if:
Religious rituals are taking significantly longer than they used to, or must be repeated a set number of times before they feel complete.
You are spending significant mental energy reviewing past actions or thoughts for evidence of sin or wrongdoing.
You are seeking reassurance about your spiritual state from family members, religious figures, or God repeatedly throughout the day.
Intrusive thoughts are consistently arising in religious or sacred contexts and causing significant distress.
You are avoiding religious spaces, people, or practices because they trigger these thoughts.
The rituals or mental checking are interfering with your daily life, relationships, or the quality of your religious practice itself.
When you do seek assessment, it is worth being specific. Not every mental health professional is familiar with OCD, and even fewer have specific experience with scrupulosity. Ask explicitly for someone who specialises in OCD and is familiar with ERP. The content of the obsessions, however disturbing they may seem to disclose, is clinically important and will not be judged by a competent OCD clinician.
Frequently Asked Questions
Is religious OCD the same as having a weak faith?
No. Religious OCD is not caused by weak faith and does not indicate it. Research consistently shows that religious OCD is more likely to develop in people for whom faith matters deeply, because OCD exploits what is most important to a person. The intrusive thoughts are a symptom of OCD, not a reflection of the person's spiritual state.
I have been told my intrusive thoughts during prayer are waswas. Is that the same as religious OCD?
The concept of waswas in Islamic scholarship (intrusive whispers that should be ignored during worship) describes something that overlaps clinically with religious OCD. Classical Islamic guidance to continue prayer without responding to these doubts is consistent with the ERP approach. However, when the waswas becomes so consuming that prayers are repeated for hours, wudu is performed repeatedly, or daily functioning is significantly impaired, this is a clinical presentation of OCD that benefits from professional treatment alongside any spiritual practice.
Does having these thoughts mean I have actually committed a sin?
No. Having an intrusive thought about something is not the same as doing it, wanting it, or endorsing it. The clinical concept of thought-action fusion describes the mistaken belief that thinking something makes it morally equivalent to doing it. This belief is part of the OCD mechanism, not a spiritual truth. Virtually all religious and moral traditions distinguish between unwanted involuntary thoughts and intentional actions. A therapist trained in OCD can help you disentangle these.
My family keeps telling me to pray more and it helps briefly, but then the thoughts come back worse. Why?
When prayer or ritual is performed in direct response to an intrusive thought (to neutralise it or restore a sense of purity), it functions as a compulsion. Compulsions provide temporary relief but teach the brain that the thought was genuinely threatening and required a response. This deepens the OCD cycle over time, which is why more prayer or reassurance is needed over time to achieve the same effect. The treatment is not more ritual. It is learning to tolerate the thought without responding to it compulsively.
Can I do ERP without compromising my religious beliefs?
Yes. ERP for religious OCD does not ask you to disrespect your faith or to act against your religious values. It asks you to tolerate intrusive thoughts without performing compulsions in response to them, and to allow the anxiety to reduce on its own. A therapist familiar with OCD and with your religious context can conduct ERP in a way that is entirely consistent with your beliefs. Many people report that their experience of religious practice improves significantly after treatment, because the OCD is no longer consuming the space that was meant for genuine connection.
Is religious OCD more common in certain faiths?
Research shows that religious obsessions affect a significant proportion of people with OCD across all major faith traditions. In highly religious societies, studies suggest religious and moral obsessions may affect up to half of all people with OCD. The specific content of the obsessions tends to reflect the person's own tradition. The fears in Hindu, Muslim, Sikh, Christian, and Jain presentations look different, but the underlying OCD cycle is the same. No religion causes OCD, but any religion can be the domain in which OCD expresses itself, particularly where faith is deeply important to the person.
Sources
International OCD Foundation: What is OCD and Scrupulosity?
Siev J et al: Obsessional cognitive styles in scrupulosity and contamination OCD — Behaviour Research and Therapy, 2025
Williams MT et al: Thought-action fusion as a mediator of religiosity and OCD symptoms — PubMed, 2013
Buchholz JL et al: Scrupulosity, Religious Affiliation and Symptom Presentation in OCD — PubMed, 2019
Psychotherapies for the treatment of scrupulosity: a systematic review — Current Psychology, 2025: doi.org/10.1007/s12144-024-06040-2
Foa EB, Kozak MJ: DSM-IV field trial: obsessive-compulsive disorder — American Journal of Psychiatry, 1995