
Contamination OCD in India
Written by Armaan Raheja, Founder of breakOCD | Clinically reviewed by Dr. Sachi Pandya, Psychologist, Mumbai
- What Contamination OCD Actually Is
- Why Contamination OCD Is Not About Being Clean
- The Many Forms of Contamination OCD
- The Cleaning Compulsion and How It Maintains the Cycle
- The Indian Context: Where Culture and OCD Overlap
- Mental Contamination: The Form You Cannot See
- Treatment: ERP for Contamination OCD
- When Your Family Will Not Cooperate
- Frequently Asked Questions
You wash your hands until they crack. You change your clothes the moment you walk in the door. You cannot eat the food someone else has touched. And you have been told this is just how you are.
If your daily life is shaped by an unrelenting need to clean, decontaminate, or avoid sources of dirt and germs that other people do not seem to notice, what you are experiencing might be Contamination OCD. It is one of the most common and most recognisable forms of OCD, and also one of the most frequently mistaken for cleanliness, religious devotion, or family particularity.
The distinction is not academic. A cultural emphasis on hygiene is not OCD. A religious commitment to ritual purity is not OCD. Contamination OCD is something specific: a pattern of intrusive fear, compulsive cleaning, and a brain that will not let you stop. This article explains what it is, why it is missed so often in India, and what the path to recovery looks like.
What Contamination OCD Actually Is
Contamination OCD is a subtype of OCD in which the obsessions centre on being dirty, contaminated, or harmed by exposure to something perceived as unclean. The compulsions involve washing, cleaning, avoiding, or otherwise neutralising the perceived contamination.
The fear is not of dirt itself in the way a child fears a muddy puddle. It is of what the dirt represents: illness, death, harm to oneself or others, moral failure, spiritual impurity. The threat feels enormous, urgent, and unbearable until the compulsion is performed.
The relief that follows the compulsion is real but brief. Within minutes or hours, the doubt returns. Was the cleaning thorough enough? Did anything get missed? Could something new have arrived since then? The compulsion is performed again. The cycle continues, and over time the threshold for what counts as contaminated drops lower and lower.
The signature of Contamination OCD is not how often a person cleans. It is the cycle: a specific intrusive fear, a specific cleaning act to neutralise it, brief relief, and the return of the doubt that demands the cleaning again.
Why Contamination OCD Is Not About Being Clean
This is the distinction that gets lost most often in Indian conversations about OCD, and it is the one that matters most.
People with Contamination OCD do not enjoy cleaning. They do not feel satisfied after a thorough hand wash. They are not perfectionists with high standards for hygiene. They are people whose lives are being controlled by a fear they cannot reason their way out of.
A person who cleans because they value cleanliness can stop when the work is done. A person with Contamination OCD cannot. The cleaning is not the goal. The cleaning is an attempt to neutralise a feeling of contamination that returns the moment the cleaning ends.
A person who washes hands after using the bathroom because of cultural practice is responding to a learned hygiene norm. A person with Contamination OCD washes their hands fifty times a day, with specific water temperatures, specific soap quantities, specific sequences, and still does not feel clean when the wash is over.
The defining feature is not the behaviour. It is the impossibility of feeling done.
Common Forms Contamination OCD Can Take
Contamination OCD presents in a wide range of forms. The specific fear varies. The underlying pattern stays the same.
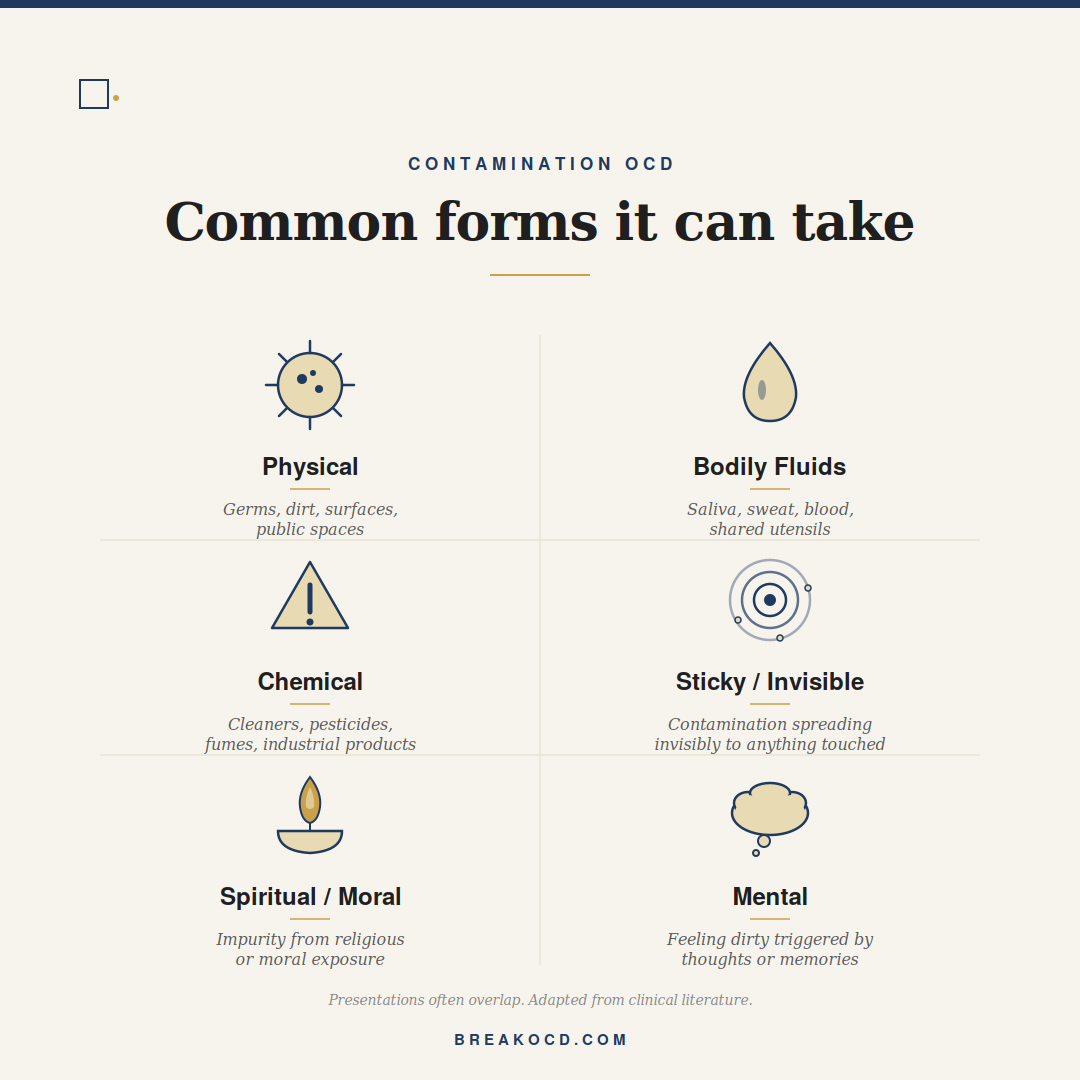
Physical contamination
The most familiar form. Fear of germs, dirt, bacteria, viruses, and physical illness. Common triggers include public surfaces, doorknobs, currency notes, public transport, restrooms, and crowded places. Compulsions involve excessive handwashing, sanitising, changing clothes, and avoiding the trigger entirely.
Bodily fluids and contagion
Fear of contamination by saliva, sweat, blood, urine, faeces, or other bodily fluids. Often triggered by shared utensils, public seating, or being touched by another person. Can escalate after exposure to news about a disease outbreak.
Chemical contamination
Fear of being exposed to harmful chemicals through household cleaners, pesticides, petrol fumes, or industrial products. Compulsions include extensive washing of imported goods, hyper-vigilance about touch, and avoidance of entire categories of items.
Sticky or invisible contamination
Fear that contamination spreads invisibly to anything the contaminated object has touched, including clothes, furniture, and family members. A single trigger can require an entire room to be decontaminated.
Spiritual or moral contamination
Fear of being made impure by exposure to something morally or spiritually wrong, such as touching a religious object after a perceived sin, or being near a place associated with impurity. This overlaps significantly with Religious OCD.
Mental contamination
A specific form in which the feeling of being contaminated arises from thoughts, memories, or interactions rather than physical exposure. There is no external trigger to clean off, but the urge to wash is strong. Mental contamination is covered in detail later in this article.
The Cleaning Compulsion and How It Maintains the Cycle
The cleaning compulsion in Contamination OCD feels like the solution. It is the mechanism that maintains the problem.
Every time the person washes in response to a contamination fear and the feared outcome does not occur, the brain draws the wrong conclusion. Instead of learning that the threat was never real, the brain learns that the washing prevented the threat. The washing therefore becomes essential. Without it, the brain expects catastrophe.
Over time, this loop tightens. The fear threshold drops. The compulsion lengthens. The avoidance expands. A person who once washed for thirty seconds now washes for ten minutes. A person who once avoided public toilets now cannot touch the doorhandles of their own home. The OCD does not stay where it began.
This is also why reassurance does not help. Telling someone with Contamination OCD that they are clean enough provides the same brief relief that a wash does, and the same return of doubt afterward. The reassurance is not addressing the mechanism. The cleaning was never about being clean. For a fuller treatment of this pattern, see our article on why reassurance makes OCD worse.
The cleaning compulsion is not the solution to the contamination fear. It is what keeps the fear alive. Every wash teaches the brain that the threat was real and the wash prevented it.
The Indian Context: Where Culture and OCD Overlap
In India, Contamination OCD is one of the most frequently missed presentations of OCD, because the surface behaviours overlap with practices that are culturally and religiously normal.
This section is the most important in this article for anyone wondering whether what they are experiencing is OCD or simply how they were raised.
The cultural emphasis on cleanliness
Indian domestic life carries a strong cultural value around cleanliness. Shoes are removed at the threshold. Hands are washed before meals. Food preparation areas are kept separate from spaces associated with the body. These are practices that have served public health and cultural identity for centuries.
These practices are not OCD. They are inherited norms. The distinction between cultural practice and Contamination OCD is not the practice itself but how it functions in the person's life.
A cultural practice has a beginning, a logic, and an end. You take off your shoes. You wash your hands. You eat. The act feels complete when it is done.
A Contamination OCD compulsion does not feel complete. The shoes have been removed but they touched the doormat and the doormat is contaminated. The hands have been washed but the tap was touched on the way to the sink. The food was prepared with cleaned utensils but the cleaning may not have been thorough enough. Nothing finishes.
Religious purity practices
Hindu, Muslim, Jain, Sikh, and Christian traditions in India all include practices related to ritual purity. Bathing before prayer, removing leather before entering temples, washing hands and feet before worship, fasting for ritual cleanliness, are all part of religious devotion practised by hundreds of millions of people.
These practices are not OCD. They are spiritual disciplines. People perform them with care and feel complete when they are done.
When a religious practice becomes a Contamination OCD compulsion, the person does not feel complete after performing it. The bathing was not thorough enough. The hands need to be washed again. The prayer cannot begin until the body feels right, and the body does not feel right. The religious framework is being used by the OCD as its content. The person is not more devout. The person is suffering.
This overlap is part of why Contamination OCD is so chronically misdiagnosed in India. To a family member, the behaviour looks like devotion. To the person experiencing it, the devotion has been hollowed out by fear.
The jhootha rules
Many Indian families have detailed customs around jhootha, the concept that food, water, or utensils touched or eaten from by another person become impure for others. These rules vary by region, by community, and by family, and most people who follow them function normally.
In Contamination OCD, the jhootha framework can expand far beyond cultural norms. The person cannot eat any food that another person has been near. They cannot share utensils even after thorough washing. They cannot drink from a glass that has touched another person's hand. The cultural rule has become a clinical compulsion, and the family often cannot see the difference.
The diagnostic confusion
In an Indian household, a person who washes their hands fifty times a day may be seen as devout, hygienic, or particular. A doctor consulted about general anxiety may not ask the questions that would reveal Contamination OCD. The cleaning behaviours fit a culturally acceptable shape, and the OCD underneath is invisible.
This is part of why diagnosis in India takes 11 to 17 years on average, according to research by Janardhan Reddy and colleagues in the Indian Journal of Psychiatry. The behaviours look like everyday cultural practice. Only when the suffering is named, the time lost is counted, and the behaviour is compared to the OCD criteria does the picture come clear.
A cultural practice has an end. A Contamination OCD compulsion does not. If the washing does not feel complete, if the doubt returns, if the act has to be done again and again, the behaviour is no longer cultural. It is clinical.
Mental Contamination: The Form You Cannot See
Mental contamination is a specific form of Contamination OCD that does not require physical exposure to anything. The feeling of being contaminated arises from a thought, a memory, an interaction, or an act, rather than from contact with a substance.
A person who has been verbally abused may feel contaminated by the words and need to bathe afterward. A person who has had an intrusive sexual thought may feel contaminated by it and need to wash. A person who has thought about a morally repugnant act may feel contaminated by the thought itself.
The compulsion is the same as physical Contamination OCD: washing, cleaning, decontaminating. But the trigger is internal, which makes mental contamination harder to identify and harder to treat without specialist support.
Research by Stanley Rachman and colleagues documented mental contamination as a distinct construct within OCD. The clinical literature has since recognised it as one of the most underdiagnosed forms of Contamination OCD, in part because the person can wash for hours without any visible reason and family members may simply not know what is happening.
If your washing is connected to something that happened in your mind rather than something you touched, what you are experiencing is mental contamination, and it is treatable.
Treatment: ERP for Contamination OCD
Exposure and Response Prevention therapy, known as ERP, is the gold-standard treatment for all forms of OCD including Contamination OCD. ERP for Contamination OCD has been one of the most extensively studied applications of the treatment, and the evidence base is strong.
ERP works by reversing the cycle the OCD has built. The person is exposed, in a graded and clinician-supported way, to the contamination triggers they have been avoiding, and prevented from performing the cleaning compulsions that follow. Over time, the brain learns what the compulsion has been hiding: the feared outcome does not require the cleaning to manage.
For Contamination OCD, ERP might involve touching a doorhandle and not washing afterward, sitting in a hospital waiting area without sanitising on the way out, sharing a utensil with a family member, or holding a memory of a contaminating event in mind without performing a mental compulsion.
The work is graded. A trained ERP therapist does not begin with the most feared scenario. They build up. Each exposure is sustained long enough for the anxiety to begin to settle on its own, which is the moment the brain starts learning the new lesson. The goal is not to stop feeling anxious. It is to stop responding to the anxiety with a compulsion.
Medication, typically an SSRI, is often used alongside ERP for moderate to severe Contamination OCD. The combination is more effective than either alone for many people. Our article on OCD and medication goes into the details of dosing, timeline, and what to ask your psychiatrist.
When Your Family Will Not Cooperate
In Indian households, Contamination OCD treatment often requires changes to family routines, and family members do not always understand why.
Family accommodation is the term clinicians use for the ways family members adjust their behaviour to manage a relative's OCD. In Contamination OCD this can be extensive: separate utensils, restricted areas of the home, repeated reassurances about cleanliness, family members being asked to bathe before entering certain rooms, or food being prepared in specific ways to avoid contamination.
These accommodations feel like care. They are also, clinically, part of what maintains the OCD. The more the family adapts to the contamination fears, the more the OCD's rules become reality, and the harder recovery becomes.
ERP treatment for Contamination OCD often involves the family in a structured way. The clinician will work with the patient and the family together to reduce accommodations gradually, in a way that supports recovery rather than triggers a crisis. This is not a sudden withdrawal of family support. It is a planned, supervised reduction of behaviours that are perpetuating the suffering.
The hardest part is often not the patient's resistance but the family's. Watching a relative tolerate distress without the relief of the compulsion feels cruel. It is, in fact, the only path to recovery. A good clinician will help the family understand why, and what their role is.
Frequently Asked Questions
Is washing my hands more than other people a sign of OCD?
Not on its own. The diagnostic question is not how often you wash, but whether the washing feels complete when it is done. If the doubt returns and the washing must be repeated, if the behaviour is taking significant time, if you are avoiding situations to prevent the need to wash, and if the cycle has been going on for some time, the pattern is consistent with Contamination OCD and worth assessing with a clinician.
How is Contamination OCD different from being hygienic?
Hygiene has a logic and an end. Contamination OCD does not. A hygienic person washes their hands and feels done. A person with Contamination OCD washes their hands and still feels contaminated, and the urge to wash again returns. The defining feature is not the behaviour itself. It is the impossibility of feeling done.
Can Contamination OCD be religious or spiritual?
Yes. Spiritual or moral contamination is a recognised form of Contamination OCD, and there is significant overlap with Religious OCD. The distinction between religious devotion and OCD is the same as the distinction between cultural cleanliness and OCD: a spiritual practice has an end. An OCD compulsion does not. When a religious practice has become a source of suffering rather than connection, it has moved into the clinical territory of OCD.
What about during a disease outbreak like COVID?
A real public health threat is not OCD. Increased handwashing, mask use, and distancing during an outbreak are appropriate responses to a real risk. Contamination OCD shows up when the response continues to escalate beyond what is needed, when the cleaning becomes ritualised, when the behaviour persists after the threat has passed, or when the person cannot bring themselves to stop even when they know rationally that they can.
Can children have Contamination OCD?
Yes. Contamination OCD often begins in childhood or adolescence. In Indian families it is frequently mistaken for shyness, fussiness, or strong cultural values around cleanliness. Parents who notice a child becoming progressively more restricted in what they can touch, eat, or do, should consider an assessment with a child mental health professional with OCD training.
Does Contamination OCD ever get better on its own?
OCD rarely resolves without treatment, and tends to expand over time as the compulsions become more elaborate and avoidance broadens. Contamination OCD is, however, highly treatable. ERP combined with appropriate medication produces meaningful and lasting reduction in symptoms for the majority of people who engage with treatment.
Will my family ever understand?
Many families come to understand, especially when the treatment process is explained to them by a clinician and they see what real recovery looks like. The change does not always happen quickly, and some family members take longer than others. What matters is that you are not alone in the process, and that the people closest to you can be helped to see that what you are experiencing is a clinical condition and not a personal failing.
Sources
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). American Psychiatric Publishing; 2022.
Rachman S. Fear of contamination. Behaviour Research and Therapy. 2004;42(11):1227-1255. pubmed.ncbi.nlm.nih.gov/15381436/
Coughtrey AE, Shafran R, Knibbs D, Rachman S. Mental contamination in obsessive-compulsive disorder. Journal of Obsessive-Compulsive and Related Disorders. 2012;1(4):244-250. www.sciencedirect.com/science/article/abs/pii/S2211364912000632
Janardhan Reddy YC, Rao NP, Khanna S. An overview of Indian research in obsessive compulsive disorder. Indian Journal of Psychiatry. 2010;52(Suppl 1):S200-S209. pmc.ncbi.nlm.nih.gov/articles/PMC3146215/
Janardhan Reddy YC, Sundar AS, Narayanaswamy JC, Math SB. Clinical practice guidelines for Obsessive-Compulsive Disorder. Indian Journal of Psychiatry. 2017;59(Suppl 1):S74-S90. pmc.ncbi.nlm.nih.gov/articles/PMC5310107/
Calvocoressi L, Lewis B, Harris M, et al. Family accommodation in obsessive-compulsive disorder. American Journal of Psychiatry. 1995;152(3):441-443. pubmed.ncbi.nlm.nih.gov/7864273/
International OCD Foundation. What is OCD? iocdf.org/about-ocd/